Neoplasms in pregnancy. Fibromyomas (Fibroids, Myomas)
The effects of gestation on fibromyomas are as follows: During pregnancy fibroids which were not noticeable before take part in the general succulency and hypertrophy of the uterine muscle and enlarge, chiefly, and perhaps only, in the first half of pregnancy. However, some authors maintain that there is no hypertrophy of the smooth muscle fibers or hyperplasia of the connective tissue stroma within fibroids during pregnancy.
Large fibroids, especially if located in the pelvis, may enlarge so much that incarceration and dangerous compression of the pelvic organs result. Aside from enlargement and increased vascularity of fibromyomas, cystic and other degenerative changes occur in most cases and in rare instances suppuration and gangrene take place.
The so-called "red degeneration" is one of the most serious changes. If it is associated with pain, fever, leukocytosis and rapid sedimentation time myomectomy or hysterectomy may be necessary. A frequent occurrence is dislocation or "wandering" and a change in the shape of the tumors. Myomas attached to the cervix respond to the upward traction of the corpus uteri and fortunately rise into the abdomen; otherwise they would block delivery.
This retraction of the tumor above the brim may occur even during labor, and the physician may be most agreeably surprised to find that what promised to be a formidable case became a simple one. The fibroid may be flattened by the growing ovum or if several tumors are present, they may be separated from each other. Subserous myomas may become twisted and necrotic or they may prolpase into the pelvis; interstitial tumors usually become more superficial; submucous fibroids, which are rare, are likely to become polypoid and may then be extruded through the cervix during the puerperium.
During labor fibroids may be crushed by the advancing head, by attempts at delivery or by a too strong Crede expression. In the puerperium myomas usually involute with the rest of the uterus. The tumors in all instances are as large as, or even larger, than they were before pregnancy, though smaller than they were during gestation. Necrosis and infection of the tumors may occur, but this accident is unusual. It is favored by the immense size of the growth, by bruising during delivery and particularly by infection, which results from wounding of the endometrium over the tumor.
The influence of pregnancy on the symptoms caused by myomas is also one of aggravation. Pain is pronounced in nearly all cases and hemorrhage, simulating threatened abortion, occurs in many. If the tumors are large the abdomen becomes enormously distended and the patient may have dyspnea as the result of pressure on the diaphragm.
The effects of myomas on pregnancy are variable. Women with such tumors are frequently sterile. Abortion occurs twice as frequently in women with fibromyomas as in other women. This is particularly true in women who have submucous tumors. Interstitial myomas have less effect and the subserous ones, unless large or near the cervix, hardly any. Placenta praevia seems to be favored by the presence of uterine tumors, probably through the concomitant changes in the endometrium. In labor fibroids usually do not cause complications unless they are impacted or adherent in the pelvis or unless the placenta is attached to the tumor. A subserous impacted myoma causes the worst difficulty, because it is less likely to be elevated by the contracting and retracting uterus. Interstitial tumors may be flattened against the wall of the pelvis so that they allow the child to pass or they may be retracted upward.
Fibromyomas exert an influence on the mechanism of labor. The uterine contractions are usually strong and painful; in fact when delivery is blocked by a tumor, rupture of the uterus may ensue. However, weak pains, even atony, may be present; abnormalities of position and presentation such as face, breech and shoulder are prone to occur; prolapse of the cord and inversion of the uterus have also been observed.
In the third stage hemorrhage is common because the distorted uterus has difficulty in compressing the vessels of the placental site. Anomalies in the separation of the placenta are especially apt to occur when it is adherent to the tumor as abnormal adherence is the rule in such cases. If the uterine cavity is distorted, the placenta may be incarcerated.
During the puerperium fibroids may obstruct the lochial flow and cause lochiometra; they always delay involution; they predispose to phlebothrombosis, and when they are gangrenous or infected the worst types of sepsis may result.
Diagnosis. The most complicated diagnostic problems are presented to the obstetrician and mistakes have been made frequently. If a woman who is known to have myomas becomes pregnant the diagnosis is not difficult and will rest on some of these points: cessation or irregularity of the menses, rapid enlargement of the uterine tumor, the development on it of a soft area, contractions of the uterine tumor and fetal heart tones. All of these may be equivocal except the last and even the fetal heart tones may be inaudible if covered by an immense tumor. If the diagnosis of an existing pregnancy is made it is usually easy to determine that there are fibroids in addition but even then mistakes have occurred because a twin, an ovarian tumor, double uterus, fibroma of the abdominal wall, fat, hematoma and Littre's hernia have been mistaken for uterine tumors.
During delivery the myomatous nodules are made prominent when the uterus hardens and, unless hidden behind the uterus, are almost always discoverable. If located in a position which causes interference with the mechanism of labor new problems are presented for diagnosis. When the uterus is emptied, its large size and the presence of nodules will easily indicate its presence. In the puerperium the corpus remains high and involution proceeds slowly. Infection of a tumor is made evident by the usual signs of sepsis.
The differential diagnosis between a large symmetric interstitial fibroid and pregnancy is sometimes difficult. Indeed it may be almost impossible to distinguish the two, even after the tumor is in the hands of the operator in the opened abdomen. (Table 23)
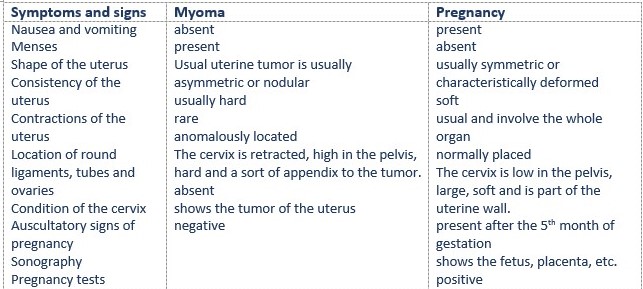
Table 23. Differentiation between Uterine Tumors and Pregnancy
After the abdomen is opened the differential diagnosis is established by the dark color of the pregnant uterus, the congested, thickened tubes and ligaments, especially the round ligaments, the presence of a large corpus luteum in one ovary, ballottement and the contractions of the tumor, which molds itself on the promontory. A fibroid is usually light in color, it rocks heavily on the promontory and it is asymmetric, as are the round ligaments.
The experienced operator usually can determine from the feel whether pregnancy exists or not. If doubt cannot be dispelled, then 1 ml (5 units) of pituitrin should be injected directly into the uterine musculature. A pregnant uterus will contract quickly and become blanched. Likewise it is justifiable to insert a wide-bore needle into the tumor. If a pregnancy is present amniotic fluid will be aspirated. Finally the tumor may be incised slowly layer by layer and, should an ovum be discovered, the wound is to be immediately sutured and the abdomen closed unless other indications exist. Pregnancy is usually not interrupted by an exploratory operation.
Prognosis. Without doubt the dangers of myomas complicating pregnancy are misrepresented by reports; this is due to the fact that only the severe cases are considered worthy of publication. Unless the tumor obstructs delivery there are few serious complications, but the fetus is more endangered.
Treatment in Early Pregnancy. It is almost never necessary to induce abortion since the majority of pregnant women with fibroids go to and through labor without difficulty. Indeed the interruption of pregnancy is difficult because of the distortion of the uterine cavity and dangerous because of the hemorrhage and the likelihood of infecting the tumors. Excessive pain and repeated and profuse hemorrhages may require treatment and, if ordinary means do not suffice, an operation may be necessary. It is best, whenever possible, to wait until or near term before operating. It may even be wise to try a test of labor because nature sometimes accomplishes wonders in getting the tumors out of the way of the child's delivery.
Therefore in the absence of unbearable pain, of severe hemorrhage, of extremely rapid growth, of great distress from overdistention of the abdomen, of signs of necrosis of the tumor, torsion or "acute abdomen," it is justifiable to wait and watch. To assist nature in elevating the tumors out of the pelvis the patient should assume the knee-chest position frequently every day. However, a laparotomy may have to be performed if a woman has a great deal of pain, impaction of the fibroid uterus, extremely rapid growth of the fibroids or excessive bleeding. Before viability it is simply best to remove subperitoneal or interstitial fibroids and to leave the pregnancy undisturbed, unless a special reason exists for amputating the uterus, such as innumerable fibroids, extensive degeneration of one or more tumors or excessive bleeding during operation. Abortion and premature labor occur in a fair proportion of cases after myomectomy. However, even if this does take place, the patient is better off because she may conceive again and she will most likely carry the gestation to term.
A surgeon should not definitely promise a patient that only a myomectomy will be performed. After opening the abdomen he may find that it is far safer for the patient to have a hysterectomy; therefore he should always have the patient's consent to do whatever he finds necessary. At term a Porro operation may be performed or, if delivery can be accomplished from below, a hysterectomy can be done a few months after delivery.
Myomectomy performed before or even during pregnancy with retention of the gestation is not necessarily an indication for cesarean section because in most instances this surgical wound heals perfectly.
Treatment near Term or in Labor. (a) Clean Cases. — Should the woman approach the end of her pregnancy a careful examination is made to determine whether the tumors will obstruct labor. It must be borne in mind that a contraction of the parturient passage caused by a fibroid is worse than the same degree of narrowing caused by a contracted pelvis, because of the possible sloughing of the tumor resulting from crushing during spontaneous, but especially operative, delivery. Should a subserous or intramural cervical myoma be so large or so firmly fixed in the pelvis that it apparently will completely block delivery, cesarean section is to be performed near term or as soon as labor has begun.
After the child and placenta are removed, an attempt should be made to raise the tumor out of the pelvis and to extirpate it. If this is impossible because the fibroid is too densely adherent or because it has grown into the broad ligaments, the uterus should be totally extirpated. Only a skilful obstetric surgeon may attempt such an operation because hemorrhage is often profuse. If there are a number of intramural tumors, it is best to perform a hysterectomy rather than multiple myomectomies.
Smaller tumors may be left for the test of labor and as a rule they will be retracted or softened and flattened so as to allow the passage of the fetus.
Operations in the uterine cavity, as version and manual removal of the placenta, may be rendered laborious by obstructing fibroid tumors and it may be necessary to push the masses up before the hand can be introduced into the uterus. Removal of a placenta adherent to a submucous fibroid may require the digging out of the two at once, but care must be exercised not to puncture the uterus. If perforation of the uterus occurs or if the extraction of the placenta fails abdominal section is indicated.
(b) Infected or Possibly Infected Cases.— When labor has been in progress for a long time, when the woman is presumably infected, or when unsuccessful attempts at delivery or reposition of the tumor have been made, the condition becomes formidable. Supravaginal amputation or total extirpation of the uterus should be performed. If the child is dead, it is best to remove the uterus in its entirety, without opening it to extract the child, the object being to prevent contact of the infectious uterine contents with the peritoneum. Even with a live child the entire uterus with the child may be removed. In definitely infected cases the danger of peritonitis should be pointed out to the husband, and the removal of the uterus advised, but in presumably infected cases an extraperitoneal cesarean section may be done with safety.
(c) During the Puerperium.
Unless symptoms are present, the myomas are not disturbed. Ergot is best omitted. Hemorrhage may require immediate operation. Sloughing, pedunculated tumors are removed per vaginam, but not too soon after delivery. If the tumors become infected expectancy is practiced until the immunities of the puerpera are developed. Precipitate laparotomy might cause fatal peritonitis. During a laparotomy for sloughing fibroids the peritoneum is to be walled off as carefully as possible and the cutting across of the pedicle, after ligation of the broad ligaments, done with the electric cautery. Drainage through the vagina should be carried out. Penicillin or the sulfonamides should be given.
Date added: 2022-12-25; views: 757;