Obstetric versions and external cephalic version
Obstetric Versions. An obstetric version is an operation by which the fetus is turned into longitudinal lie for delivery.
The following obstetric versions are differentiated: external version, classical internal version with fully dilated cervix, and internal version with incomplete dilation of the cervix (Brexton-Hicks version). Brexton-Hicks version is not used in modern medicine.
External cephalic version. The external cephalic version is used in transverse or oblique lie of the fetus. Sometimes breech presentation may be another indication to external version.
The external version in transverse and oblique presentation should be performed in hospital in the 35th-36th week of pregnancy.
The conditions permitting the external version are:
- good mobility of the fetus (the amniotic fluid has not escaped);
- manageable abdominal wall;
- the uterine tonus is normal;
- normal size and architecture of the maternal pelvis;
- normal size of the fetus;
- fetus is alive;
- good health of the mother;
- pregnant agrees to the operation.
Oblique presentation can be corrected without any external manipulation: the patient is offered to lie on her side (incompliance with the position of the large presenting part of the fetus). If it fails, the fetus is turned externally.
Contraindications are:
- hemorrhages during this pregnancy;
- threatened abortion during this pregnancy;
- spontaneous abortion or premature labor in the previous history;
- hydramnios, oligohydramnios;
- multiple pregnancy;
- contracted pelvis;
- pregnancy with EPH-complex, cardiovascular diseases, etc;
- congenital anomalies of the uterus, tumors;
- adhesions in the abdominal cavity after any operations;
- the scar on the uterus after cesarean section, conservative myomectomy;
- contracted vagina (because of scars).
The fetus head is usually brought down by external version. If the head is located near the pelvic inlet, it is brought down, and vice versa, if buttocks are closer to the pelvic inlet, the fetus is turned with its podalic end toward the pelvic inlet.
The operation should be performed without anesthesia.
Technique: The patient lies in dorsal position, on a firm bed. Her bladder and rectum are empty. The woman bends her legs and the physician sits on her right side, face to face. One hand of the physician rests on the fetal head and the other one on the fetal buttocks. By careful manipulations the head is moved toward the pelvic inlet and the buttocks towards the fundus of the uterus. When the fetus is turned into the longitudinal lie, measures are taken to prevent its return to malpresentation; two pads (rolled up bed-sheets) are placed by sides of the fetus (its back and the smaller parts flexed on the chest and abdomen) and bandaged in this position without pressing tightly on the maternal abdomen (Fig. 152, 153).
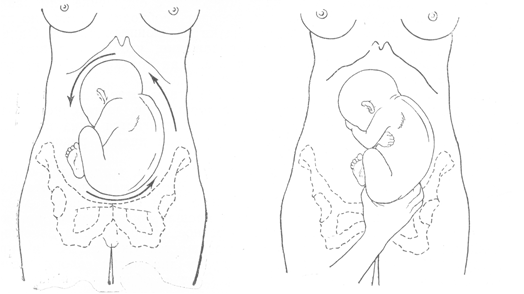
Fig. 152. External version of the fetus
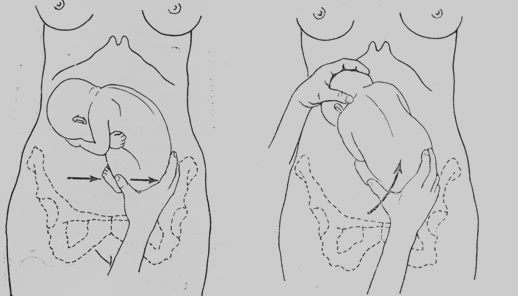
Fig. 153.External cephalic version of the fetus: continuation
Classic Podalic Version with a Fully Dilated Cervix (Internal Version). Indications for podalic version are as follows:
- transverse lie of the fetus (if external version fails);
- deflexed presentation and asynclitism (brow presentation, face presentation, posterior face presentation, posterior asynclitism);
- prolapse of the umbilical cord and smaller parts of the fetus in cephalic presentation;
- complications and diseases endangering the mother and fetus (premature separation of placenta, etc).
Contraindications are:
- neglected shoulders;
- threatened rupture of the uterus;
- rupture of the uterus;
- the scar on the uterus after cesarean section or conservative myomectomy;
- cephalopelvic disproportion.
The requisite conditions are the following:
- full dilation of the cervix;
- intact membranes or just escaped amniotic fluid;
- the fetus is fully mobile in the uterine cavity;
- absence of cephalopelvic disproportion (absence of pronounced contracture of the pelvis).
General anesthesia is necessary in this operation. The operation should be performed in sterile conditions.
Technique. The operation comprises the following manipulations: introduction of the operator’s hand into the uterus, identification of the leg, grasping the leg, and version proper.
A repeated external and vaginal examination is required before the operation in order to determine exactly the position and presentation of the fetus, degree of cervix dilation, and other important factors.
Introduction of the operator’s hand. Usually the right hand has to be internal, as it is more skilful. However some surgeons prefer the left hand to be internal. The rule may be used: when the fetus is to be turned from transverse lie into longitudinal one, the internal hand should correspond to the pelvic end of the fetus (left hand to the left and right hand to the right position of the fetus).
The external hand is used to open the pudendal cleft, and the internal hand shaped into a cone is introduced into the vagina and moved towards the uterine cervix (the back of the hand should face the sacrum). When the fingers reach the cervical os, the external hand should be placed on the uterine bottom. The fetal membranes are then ruptured and the hand is moved farther into the uterus (Fig. 154).
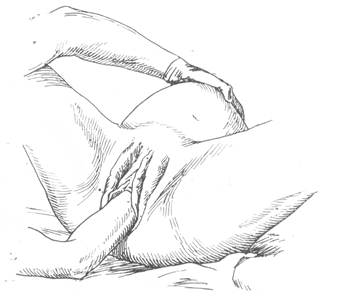
Fig. 154. Classic podalic version with fully dilated cervix (internal version). The internal hand is introduced into the vagina for grasping the leg
Identification of the leg. A leg lying near the abdominal wall of the mother should be found for version from the longitudinal presentation. The choice of the leg in transverse presentation depends on type of the fetus position: the inferior leg should be grasped if the fetus back is turned to the maternal abdominal wall. If the fetus back is turned to the maternal spine, the superior leg should be grasped.
To identify the leg, the hand feels the side of the fetus and slides from the armpit to the pelvic end, and further by the thigh to grasp the leg. The external hand should assist by moving the pelvic end down toward the internal hand of the operator (Fig. 155).
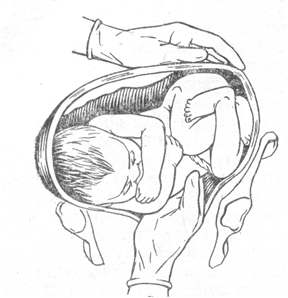
Fig. 155. Internal version. Identification of the leg
Grasping the leg. This can be done by two methods:
- The leg is grasped by the entire hand, i.e. four fingers are placed on the anterior part of the leg while the thumb is placed on the calf to reach the popliteal fossa (Fig. 156).
- The index and the middle fingers grasp the malleolus, while the thumb supports the sole. The former method is however more reliable (Fig. 157).
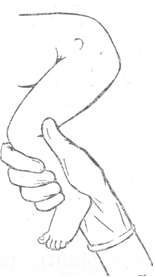
Fig. 156. Internal version. Grasping the leg: the leg is grasped by the entire hand
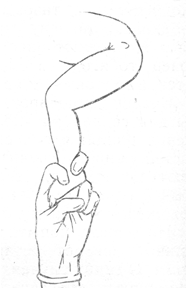
Fig. 157. Internal version. Grasping of the leg: the leg is grasped by two fingers
Version proper. After a firm grip is placed on the fetal leg, the external hand moves the fetal head upwards, i.e. to the fundus of the uterus. During the course of this manipulation, the internal hand pulls the leg outside the vagina. The version is considered complete when the leg is extracted from the pudendal cleft to the knee (Fig.158).
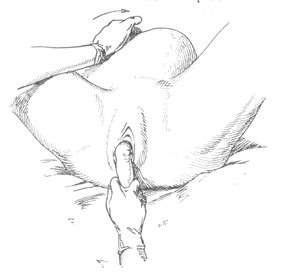
Fig. 158. Internal version. The leg is extracted from the pudendal cleft to the knee
This indicates that the fetal assumes the longitudinal position. The arm may be prolapsed with the discharge of amniotic fluid in transverse presentation. The prolapsed arm should not be corrected but only pulled by a sterile gauze strip towards the symphysis. As the fetus is then turned, the arm retracts spontaneously.
Date added: 2022-12-17; views: 1135;