Extraction of the fetus. Extraction by the leg or legs
Whenever complications endangering the mother and the fetus arise, labor in breech presentation should be ended by extraction of the fetus. This method is also used after the podalic version with a fully dilated cervix.
Extraction differs from manual assistance. Manual assistance in breech presentation is given after spontaneous delivery of the fetus to the lower angle of the shoulder-blades, its objective being to deliver the arms and the head.
Extraction of the fetus by the pelvic end is an operation in which the entire fetus, beginning with the legs, is extracted. The operation is performed by the hand only.
Indications:
- Severe diseases requiring urgent termination of labor (eclampsia, heart diseases, etc);
- Occurrence of asphyxia of the fetus;
- After the classical podalic version.
Requisite conditions:
- Fully dilated cervix;
- Rupture of the fetal membranes;
- Absence of cephalopelvic disproportion.
The fetus is extracted by one leg (in single footling) or by two legs (in double footling presentation).
Extraction by the leg or legs. If the presenting leg is in the vagina, it is extracted by two fingers. The leg is grasped in the following way: the thumb is placed on the calf, and the other four fingers — on the anterior surface of the leg. The leg may be grasped by both hands: both thumbs are then placed on the calves. This grip on the leg prevents its fracture (Fig. 159).
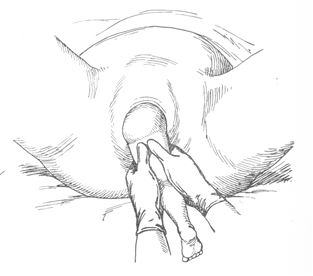
Fig. 159. Extraction by the leg: the leg is grasped by both hands
The downward traction should then be applied to the leg. As the leg appears from the birth canal, the operator’s hand should move farther along the infant leg toward the pudendal cleft. The downward traction should be continued until the forthcoming buttock and the iliac bone are brought beneath the symphysis. The forthcoming thigh is then grasped by both hands and lifted slightly (Fig. 160).
The fatal body is thus flexed and the aftercoming buttock is delivered over the perineum.
No attempts should be taken to free the aftercoming leg for it may be fractured; the leg will be delivered spontaneously during further traction.
After the second buttock has been delivered, one hand should grasp the anterior thigh (the thumb being positioned on the sacrum), while the index finger of the other hand should engage the posterior groin of the fetus with the thumb resting on the sacrum (Fig. 161). The other fingers should be pressed against the palm. With the hands thus gripped on the buttocks, the operator continues the downward traction.
After the aftercoming leg is delivered, it is taken by the hand in the same manner and the fetus is extracted to the navel. The cord is checked for the absence of tension, and the fetus is extracted to the lower margin of the shoulder blades. Now the arm and the head are freed by manoeuvres as specified for manual assistance.
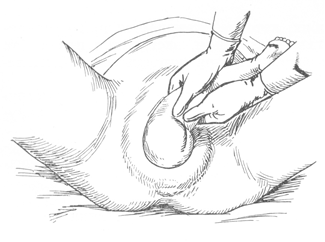
Fig. 160. Extraction by the leg: the forthcoming thigh is grasped by both hands and lifted slightly
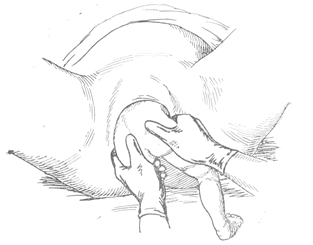
Fig. 161. Extraction by the leg: pulling the fetus till the navel
Extraction by the Groin. Extraction of frank breech presentation begins with inversion of one index finger into the anterior fetal groin (Fig. 162).
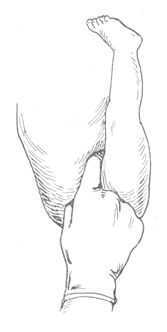
Fig. 162. Extraction by the groin
The traction is continued until the anterior buttock is freed and the iliac bone is brought beneath the pubic arch. Traction is only applied when the uterus contracts, in order to add to the traction effort. The other hand should assist by grasping the wrist of the operating hand (Fig. 163).
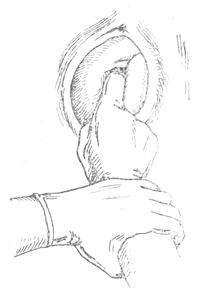
Fig. 163. Traction by the groin
When the anterior iliac bone is brought beneath the symphysis, the direction of traction should be changed to the upward one. The fetal torso is flexed and the posterior buttock is disengaged. The index finger of the other hand should now be inserted into the other groin. Traction is continued until the fetus is delivered to the lower margin of the shoulder blade. The legs are freed spontaneously.
The arms and the head are freed as in manual assistance.
Extraction by the groin is one of the most difficult obstetric operations. The operating hand is quickly fatigued, the buttocks move slowly. It is especially difficult to extract the fetus with a high position of its buttocks.
Possible complications. The following complications may occur in extraction (manual assistance): spasm of the uterine cervix, extension of the arms, posterior presentation, etc.
In order to remove the spasm of the cervix os, the operation is performed with anesthesia. Spasms may be prevented by giving (before operation) 1 ml of a 1% papaverine solution and 1 ml of a 0.1% atropine solution.
In order to correct the arm (when it is extended), four fingers should be inserted into the vagina and the arm pulled down along the face and chest (the fetus “washes” its face).
Extraction of the fetus is also difficult with persistent posterior position (the chin turns towards the symphysis and the occiput towards the sacrum). To disengage the head in posterior position, the following manipulations are required. The tip of the index finger is placed into the fetal mouth to flex the head, while the other hand of the operator should extract the fetus until the nose bridge (fulcrum) is brought beneath the symphysis.
The torso of the fetus is then bent anteriorly (toward the mother’s abdomen) and the head is delivered over the perineum. If the head is extended and the finger fails to reach the mouth, the torso of the fetus should be flexed on the mother’s abdomen, while the other hand of the operator should grip the shoulders with the fingers (like a fork) to assist extraction of the fetus. The head passes the pelvis by its vertical diameter, the fulcrum being the region of the hyoid bone.
Date added: 2022-12-17; views: 935;