Eye Infections. Obesity
Serotypes 8, 11, 19, and 37 can cause epidemic keratoconjunctivitis (EKC) in which the conjunctiva becomes infiltrated, chemotic, and hyperemic. Sporadic keratoconjuctivitis has been observed, but the major epidemics have been associated with Ad19 and Ad37. Cases have been documented worldwide including in North America, Asia, and Europe.
Transmission occurs through direct contact with eye secretions from an infected person as well as through contact with contaminated surfaces, eye instruments, ophthalmic solutions, towels, or hands of medical personnel. Trauma to the eye can increase a person’s risk of infection. Outbreaks have involved mostly adults.
The first identified outbreak occurred in 1955 and involved shipyard workers in Hawaii exposed to rust and paint chips. The workers became infected with Ad8 (‘shipyard eye’ or ‘shipyard’ conjunctivitis). Other documented outbreaks of keratoconjunctivitis due to adenoviruses have involved ophthalmic solutions and a roller towel used for drying faces and hands.
Outbreaks of EKC are commonly reported from offices of ophthalmologists. Spread is thought to occur through insufficient sterilization of equipment or contact lenses, direct manipulation of the eye, or by use of eye solutions and ointments. Secondary spread between children and family members has also been documented, although direct inoculation into the eye appears to be necessary for disease.
Infections of the conjunctiva refer to a clear membrane that coats the inner aspect of the eyelids and the outer surface of the eye. Conjunctivitis can occur sporadically or occur in large groups. Often, follicular conjunctivitis is contracted by swimming in inadequately chlorinated swimming pools or in lakes during the summer.
The first documented outbreak of conjunctivitis was in 1955, as adenovirus was isolated from swimmers at a local pool. Most cases result in only mild illness and complete recovery. Adenoviruses 3 and 7 are the most commonly isolated species, although many other serotypes have been associated with this syndrome.
Obesity. There is accumulating evidence that several viruses may be involved in obesity in animals and humans. Studies in chickens, mice, and nonhuman primates indicate that adenovirus type 36 can cause obesity. Obese humans have a higher prevalence of serum antibodies to adenovirus 36 than lean humans.
Other adenoviruses are capable of causing obesity in animals, but no correlation with antibodies has been demonstrated. The metabolic and molecular mechanisms of how adenovirus infections cause obesity are not precisely understood; however, increases in food intake alone cannot explain the observed increases in adiposity (tendency to store fat), suggesting that adenovirus 36 induces metabolic changes.
One mechanism appears to be that adenovirus 36 influences the differentiation of preadipocyte cells and/or the accumulation of lipids by adipocytes (cells that accumulate fat in the body).
Morbidity and Mortality.Since adenovirus is not a reportable disease agent, there are no national or population-based morbidity and mortality figures available; most of the epidemiological data come from the study of select populations who appear to be most affected by adenovirus exposure. These include children in institutions such as hospitals and day care centers, military recruits, immunocompromised individuals, and groups of families.
Adenovirus infections were common among military personnel in the 1950s and 1960s, with as many as 10% infected. They were also responsible for 90% of pneumonia hospitalizations. The impact of adenoviruses subsided with the implementation of a vaccine; however, the sole vaccine manufacturer ceased its production in 1996. Subsequently, morbidity ratios have again increased to 10-12% and deaths have been observed in previously healthy military recruits.
Impact on the Immunocompromised.The severity of disease resulting from an adenovirus infection depends on the host’s immune system status. Therefore, adenovirus infections in immunocompromised hosts (including HIV-infected patients and transplant recipients) have been well documented. While nonenteric adenovirus infections produce usually moderate disease in people with normal immune systems, the immunocompromised are at higher risk for serious and possibly fatal disseminated disease.
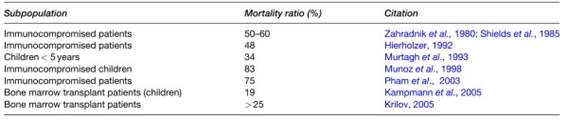
Table 3. Mortality ratios associated with adenovirus illnesses in subpopulations
Though adenovirus infection may result in mild or asymptomatic infections in the immunocompromised, the virus can disseminate into any body system and cause pneumonitis, meningoencephalitis, hepatitis (especially in liver and bone marrow transplant patients), and hemorrhagic cystitis (especially in kidney transplant patients). The disease may progress to death. The enteric adenoviruses are rarely isolated from immunocompromised patients with gastroenteritis or diarrhea (Table 3).
Date added: 2024-02-03; views: 715;