Adolescent Nutrition. Malnutrition
Malnutrition. Adolescents have the greatest nutritional requirements of any age group, mainly to support their growth spurt. Teenagers who do physical labor or have certain chronic diseases have even higher nutritional needs. When resources are scarce, adolescents may not have access to enough food. In some cultures, to preserve provisions, females eat last and eat least.
Longstanding malnutrition causes adolescents to be thin and their height stunted. Undernutrition is defined by the WHO as having a body mass index (BMI, measured by weight in kg divided by height in m2) less than the 5th percentile of the population of the same age. Undernutrition in adolescence is most common among youth in Southeast Asia, such as India and Nepal, where overcrowded conditions and poverty are common. Malnourished children chronically lack calories.
At this critical time in cognitive maturation, brain development can be adversely affected by persistent energy deficiency. These children are also commonly deficient in micronutrients (trace minerals, essential amino acids, vitamins, and essential amino acids).
Micronutrient deficiency is one of the most easily preventable causes of death and disability. Iron deficiency, the most common micronutrient deficiency among youth, is associated with anemia, poor cognition, and reduced work capacity. Inadequate protein intake, vitamin deficiencies (A, B, D, E, K), and inadequate iron, zinc, and copper can lead to inadequate immune functioning and can increase risk of infection and disability. Nutritional programs such as homestead production, plant breeding, food fortification, and supplementation do exist and offer some benefit, but lose effectiveness when not holistic or incorporated into larger social development programs.
Women’s nutritional needs rise during pregnancy, which can worsen their already poor nutritional status. Malnourished females suffer more obstetric complications; delivery may become obstructed due to their small pelvis. Prenatal folate deficiency is associated with neural tube defects and low birthweight. Children of malnourished young women are at higher risk for growth retardation, cognitive delays, infection, disease, and death.
Efforts to improve nutritional status in the chronically malnourished generally cause weight gain, but may not cause a catch-up in height or cognitive development, especially if a teenager has already completed puberty. Short adult heights are associated with reduced earning potential and working capacity.
Obesity. Obesity is an epidemic in the industrialized world, and increasingly in developing areas. Obesity and overweight are characterized by excess body fat, caused by a discrepancy between the consumption and utilization of caloric energy. The definitions for adolescent obesity and overweight vary. In the United States, most recently BMI greater than the 95th percentile for age is termed ‘overweight,’ and BMI greater than the 85th percentile is termed ‘at risk for overweight.’
Cole et al. and the International Obesity Task Force (2000) sampled children from six countries and determined internationally based BMI cutoff values for overweight and obesity based on the expected trajectory to be an overweight or obese adult (defined by BMI of 25 or 30, respectively). Lissau et al. and the Health Behavior in School-aged Children Obesity Working Group (2004) compared BMIs derived from the self-reported height and weight in teenagers in 14 countries to the group’s reference standard (Figures 4 and 5).
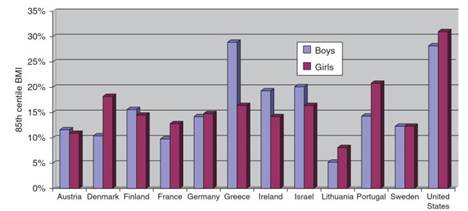
Figure 4. Prevalence of BMI at or above 85th percentile in 15-year-olds, selected countries. Adapted from Lissau I, Overpeck MD, Ruan WJ, etal. (2004) Body mass index and overweight in adolescents in 13 European countries, Israel, and the United States. Pediatric and Adolescent Medicine 158: 27-33. Copyright © 2004, American Medical Association. All rights reserved
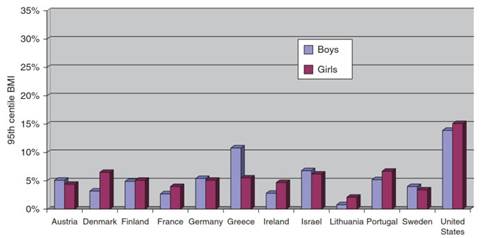
Figure 5. Prevalence of BMI at or above 95th percentile in 15-year-olds, selected countries. Adapted from Lissau I, Overpeck MD, Ruan WJ, etal. (2004) Body mass index and overweight in adolescents in 13 European countries, Israel, and the United States. Archives of Pediatric and Adolescent Medicine 158: 27-33. Copyright © 2004, American Medical Association. All rights reserved
Globalization has brought Western diets to most of the world, making obesity the most common disease of childhood worldwide. In many developing countries, such as in Southeast Asia, obesity and malnutrition coexist; as societies are urbanized and modernized, their populations begin to consume high-calorie, high-fat, processed foods and have a sedentary lifestyle, all of which can contribute to obesity.
The highest adolescent obesity rates are found in the Americas and Western Europe, particularly in the United States; the lowest rates are in the former Soviet Union and sub-Saharan Africa where food shortages still exist.
The causes of adolescent obesity are multifactorial. During puberty, teenagers normally gain weight before their peak in growth velocity, and females generally continue to gain weight during puberty. Adolescents have an increasing amount of control over their own diets, yet oftentimes lack the judgment to make good nutritional choices. Unfortunately, for many teenagers, this entails choosing calorie- dense foods that lack nutritional value instead of those high in fiber and low in fat such as fruits and vegetables.
Such processed ‘fast foods’ are readily available, cheap, and often sold and eaten in large quantities. Teenagers who eat quickly or eat during other activities such as watching television are more likely to be obese. Those who are busy in school or at work may skip meals, slowing their metabolism. Low levels of physical activity compound these nutritional issues; in the modern world, many young people drive cars and play computer games instead of walking or engaging in physical recreation. Formula feeding during infancy and intrauterine growth retardation have also been associated with childhood obesity.
The consequences of adolescent obesity are extensive. Overweight adolescents are more likely to have poor self-esteem, and to be teased by their peers or family. Many youth deal with the harassment by eating more, often privately, causing a maladaptive cycle. They may skip meals in an effort to reduce calorie intake, which often leads to a pattern of under-eating and binging, causing them to gain more weight. Obese youth are more likely to have diabetes, fatty liver disease, asthma, and obstructive sleep apnea. A large proportion of obese adolescents become obese adults, as they develop eating habits and sedentary habits that may last a lifetime. Overweight adults are more likely to suffer from hypertension, atherosclerosis, cancer, osteoarthritis, and gall bladder disease, and are more likely to die prematurely.
There are few randomized controlled trials evaluating interventions to prevent adolescent obesity, most of which have not shown any effect. Treatment of obesity has predominantly focused on interventions at the personal level, such as encouraging less television viewing and controlling portion size. Many of these studies have entailed only brief periods of intervention and support, which may not translate into sustainable changes in lifestyle. Some centers have begun to perform gastric bypass surgeries on adolescents, a procedure previously reserved for morbidly obese adults.
Adolescents often lack the motivation and selfconfidence to alter their routines. They are more vulnerable to pressure from peer groups or family members who make unhealthy nutritional choices. Teenagers may benefit from a supportive environment in which their families and peers improve their diet and activity level. Programs that take a holistic approach toward an overweight adolescent, encompassing social and psychological issues, may be more successful. More research is certainly needed to find useful interventions to prevent and treat obesity in adolescents.
Sexual Health. Early Sexual Activity
Early Sexual Activity. Despite many cultural taboos, a large proportion of adolescents are sexually active. According to the Guttmacher Institute, 68% of adolescents in the United States and 72% in France have had premarital sex by age 20; 43% of women in sub-Saharan Africa and 20% of 20-year- old women in Latin America have had premarital sex (Guttmacher Institute, 1998).
Early sexual activity has numerous consequences, including pregnancy and the spread of sexually transmitted infections including HIV/ AIDS. As puberty tends to start earlier and the average age of marriage rises, adolescents today are more likely than ever to have premarital sex.
Sexual activity that is voluntary in which participants are protected against sexually transmitted infections and pregnancy likely minimizes physical and psychological risk. Sexual attraction is a normal part of maturation, and is necessary for propagation of the species.
Despite this fact, many cultures hold a repressive attitude about intercourse, particularly among young unmarried adults. Experimentation is common in many aspects of adolescents’ lives, including sexual activity, and so many youth may participate in vaginal, anal, or oral sex.
Sexual activity early in adolescence can also be associated with coercion and abuse, and other risk behaviors such as substance use. Adolescents often lack the selfconfidence to confront their partners and refuse to have sex, especially when their partner is older. In societies where femininity is defined by obedience and innocence, and virginity is equivalent to virtue, the sexual health of young women can be compromised for those who are less likely to access family planning services and be tested for infections including HIV.
Pregnancy. Pregnancy in adolescence is a common occurrence in the industrialized and developing world, with a myriad of consequences for young women and men and their communities. There are more than 14 million births to adolescents each year, with the vast majority (>90%) occurring in developing countries in sub-Saharan Africa, Asia, and Latin America. On average, worldwide adolescent fertility rates have dropped as young women postpone childbearing, especially in North Africa and the Middle East. Fertility rates in sub-Saharan Africa have not fallen to the same degree (Table 2).
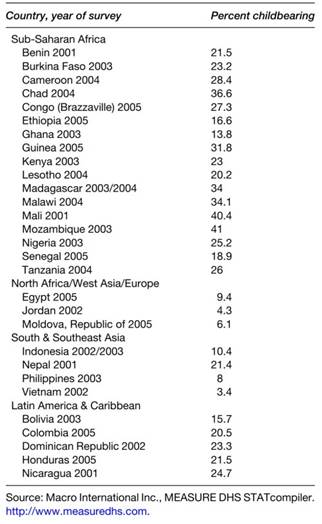
Table 2. Percentage of females aged 15-19 years who are pregnant or have had a child
In most regions, adolescent pregnancy is associated with risk behaviors, including having multiple sexual partners, sexually transmitted infections, failure to use contraception, and alcohol use. The relationship between early pregnancy and poor economic or educational opportunities is increasingly being recognized.
Most pregnancies during adolescence are unwanted or unplanned, with teens typically lacking resources and skills available to older mothers. Access to safe and legal abortion services is another important factor in determining birth rates. In regions of the world such as Scandinavia, where adolescent sexuality is accepted as a normal part of human development and where teens have access to contraception and abortion, birth rates are lowest.
Other regions of the world fare more poorly. In countries such as the United States, where mixed messages are portrayed to teenagers regarding sexuality and access to contraceptive and abortion services is more limited, birth rates are higher than in many other industrialized countries despite having similar rates of adolescent sexual activity. Importantly, access to contraception is a key factor in determining the adolescent birth rate, not regional differences in rates of early sexual activity.
Adolescents use contraception at lower rates than adults. The proportion of adolescents having knowledge of their contraceptive options is rising, especially in Latin America, yet a significant proportion of adolescents do not have a basic understanding of sexual health and pregnancy. Adolescents can theoretically safely use any form of birth control that adults can. Lack of access to family planning services is especially prevalent among the poor and uneducated.
Teenagers tend to be risk takers and may have an invincible attitude, thinking they cannot get pregnant. They may not have the judgment to plan ahead to bring and use contraception regularly. The cost of birth control may be prohibitive; teenagers may not have health insurance or may be unwilling to use their parents’ insurance due to privacy issues. Fear of disapproval from society or health-care workers can also lead to young people to not seek birth control.
Early marriage is associated with adolescent pregnancy. One hundred million girls under the age of 18 will get married over the next 10 years, usually to older partners. Child marriage is becoming less common worldwide, except in South America. Poor, uneducated youth tend to marry early, often for financial and/or cultural reasons. Many young women, especially those in regions where resources are scarce, may have sexual relationships outside of marriage with older men (‘sugar daddies’) in order to receive gifts or support themselves financially.
These relationships have an unequal power structure, and young teenagers may feel uncomfortable asking their partners to use contraception. Within the marital relationship, sex tends to be unprotected. Older men may seek out young women because they are more vulnerable to coercion and less likely to be infected with HIV; these females are correspondingly at higher risk to acquire sexually transmitted infection from their older partner.
Girls who get married at an early age tend to not finish their secondary education, which adversely affects their earning capacity and potential for financial independence. Young women are more likely than adults to have their first child very soon after they wed, to not space their children, and to have a larger number of children. These behaviors create unfavorable health outcomes for their offspring.
Childbearing during adolescence has significant effects. Pregnant teenagers are less likely to finish school, either because they drop out of school to avoid the stigma or because they are expelled to prevent them from being a role model for other young women. Unmarried pregnant adolescents may be outcasts in their community, further marginalizing them. They represent lost workforce for their community, hindering economic development of their area. Their children further rapid population growth, straining the community’s financial infrastructure.
Pregnant teenagers are less likely to access prenatal care because they are less experienced and educated, and more frequently attempt to hide their pregnancy than adult women. Lack of prenatal care further jeopardizes a young pregnant woman’s health as well as her baby’s.
Pregnancy-related complications are among the most common causes of death for young women aged 15 to 19 worldwide. Adolescents in the developing world are more likely to have obstetric fistulas, which can cause a lifetime of sexual dysfunction, urinary obstruction, and poor selfimage. Pregnant teenagers are twice as likely to die during childbirth, often from an abrupted placenta, hemorrhage, or obstruction.
Pregnant youth are at high risk for physical abuse, often from their partner. In turn, parenting adolescents are more likely to physically abuse their own children, often in desperation when feeling overwhelmed from a lack of emotional or financial support. Infants born to adolescent mothers are more likely be drug- or alcohol-exposed, born prematurely at low birthweight, and die within the first year of life.
Teenagers often lack the cognitive and emotional maturity to effectively parent their children. Delaying childbearing for even a few years to allow the body to mature and their economic and educational position to improve can drastically improve health outcomes for adolescents and their children.
Abortion. Up to 4 million abortions are performed each year on adolescent girls. In regions where abortion is legal, abortions are generally very safe and performed by licensed practitioners. When abortion is illegal or difficult to access for young women, most procedures are performed by unskilled technicians, often in unsanitary conditions.
Death from abortion is one of the major causes of maternal mortality worldwide; the majority of complications from abortions occur in adolescents. Due to social pressures, adolescents may keep their pregnancies secret, and delay seeking an abortion, making the procedure riskier. They also are less likely to seek care when complications do occur, placing them at further risk for injury or even death.
Sexual Coercion. Nonconsensual sex is common during adolescence, especially in young females and those who are institutionalized or homeless. Most often, the perpetrator is someone known to the child, such as a peer, romantic partner, or authority figure.
Child marriages, especially those that are arranged, are associated with early nonconsensual sex. It is difficult to find reliable data regarding the frequency of forced sexual relations among adolescents because the vast majority of cases are never reported. Victims often feel ashamed or guilty. In many regions, laws against nonconsensual sex do not exist or are not enforced.
During this formative time, rape can have devastating effects on a young person’s development. These youth are more likely to be depressed, commit suicide, have poor self-esteem, abuse substances, and engage in risky sexual behavior, including having multiple sexual partners, unprotected sexual activity, and prostitution. They are less likely to finish school, and may be ostracized from their community.
Adolescents under severe financial strain, such as those who are homeless or refugees, may resort to selling sex in order to survive. Youth involved in the sex industry are at high risk for physical abuse, psychological problems, substance use, pregnancy, sexually transmitted infections, HIV/AIDS, and early death.
Sexual tourism has become a worldwide phenomenon, particularly in countries such as Thailand and Brazil; over 1 million children and adolescents are recruited or forced into this labor every year. The highest demand appears to be for those aged 12 to 16 years. Tourists typically travel from wealthier countries to poorer regions, where they are less likely to be prosecuted.
Sexually Transmitted Infections. Adolescents and young adults carry a disproportionate burden of sexually transmitted infections (STIs), including trichomonas, chlamydia, gonorrhea, herpes, syphilis, and human papilloma virus. STI rates are highest among those aged 19 to 24; those 15 to 19 have the second- highest rates. Each year, 1 in 20 adolescents contracts an STI. STI prevalence rates are not always systematically tracked, but seem to vary across regions and are highest in developing countries.
Adolescents are at high risk to acquire STIs for a variety of reasons. Persistence of the cervical ectropion in young women confers on them an increased risk of infection with chlamydia and gonorrhea. Despite the fact that condoms prevent transmission of most STIs, teenagers fail to consistently use barrier contraception due to cost, poor access, or an inability to stand up for their health needs in a relationship where power is imbalanced.
Many youth believe that condoms mark them as already infected, imply distrust of their partner, or reduce pleasure. Other teenagers have never had the proper health education to understand the importance of condom use in the protection of their reproductive health.
Unprotected sexual activity with multiple sexual partners often occurs within the context of other risk-taking behaviors, such as alcohol or drug use. Those who are incarcerated, homeless, or work in the sex industry are at highest risk for acquiring STIs.
Infection with gonorrhea or chlamydia can cause chronic abdominal pain, pelvic inflammatory disease, enhanced HIV transmission, ectopic pregnancy, abortion complications, and infertility. Infection during pregnancy can cause miscarriage or preterm labor. Human papilloma virus causes anogenital warts and cancers of the anus, vagina, and cervix.
Many adolescents, especially those in developing countries, lack access to Papanicolaou smears, which are critical in the prevention of cervical cancer. Sexually associated infections such as bacterial vaginosis appear to enhance HIV transmission. Syphilis causes permanent neurotoxicity. Herpes simplex virus leads to social isolation, painful outbreaks, and perinatal complications including neonatal encephalitis, seizures, and death.
STIs are often asymptomatic for extended periods of time; unscreened adolescents may unknowingly spread infection to a number of partners. Fortunately, some STIs are easily diagnosed and treated. However, even when symptomatic, an inadequate number of adolescents actually seek care. Teenagers may be less likely to recognize STI symptoms because they are uneducated. Seeking medical attention for screening during an asymptomatic period as well as when symptomatic takes maturity and financial resources that many teenagers lack.
Date added: 2024-02-03; views: 917;