Regional HIV Surveillance Data
The HIV epidemic has developed distinctly in different regions. Generalized epidemics occur when the general population HIV prevalence reaches 1% or more, and concentrated epidemics are described as an HIV prevalence of 5% or more in high-risk groups.
Sub-Saharan Africa: Overview. In 2006, HIV and AIDS continue to have a devastating effect on sub-Saharan Africa which is home to 24.7 million people living with HIV and 63% of all HIV-infected individuals in the world. Approximately 2.8 million people became newly infected in sub-Saharan Africa in 2006, and approximately 2.1 million people died from HIV in this same year. Women are more likely to be infected than men in this region, and 59% of all HIV- infected persons are estimated to be female (Figure 7) (UNAIDS/WHO, 2006).
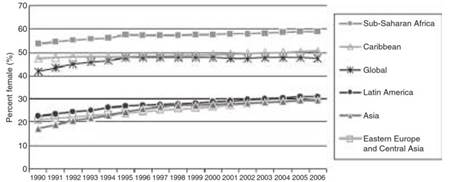
Figure 7. Percent of adults greater than 15 years of age living with HIV who are female, 1990–2006. Reproduced with kind permission from UNAIDS/WHO (2007) AIDS Epidemic Update 2006. Geneva: UNAIDS/WHO
Southern Africa. Within sub-Saharan Africa, Southern Africa has the highest burden of disease, accounting for 32% of HIV-infected individuals and 34% of AIDS deaths in the world. All countries of Southern Africa continue to increase in prevalence, except Zimbabwe, where HIV seroprevalence among adults has reduced to 20.1% from 22.1% in 2003. A decrease in HIV prevalence was reported in antenatal clinics in Zimbabwe from 30-32% in 2000 to 24% in 2004.
Swaziland has the highest adult prevalence of HIV globally at 33.4%, and South Africa has the second greatest number of HIV-infected persons among all nations in the world after India. Across Southern Africa, the death rate from AIDS significantly increased in both men and women between 1997 and 2004, despite increased antiretroviral availability and use.
East Africa. Overall, HIV prevalence has been stabilizing or decreasing in this region of Africa. Kenya, Tanzania, and Rwanda have all shown a decline in prevalence over the last several years. In Kenya, adult HIV prevalence decreased from 10% in the late 1990s to approximately 6% in 2005 (Kenya Ministry of Health, 2005), and in Tanzania, adult HIV prevalence decreased from 8.1% to 6.5% between 1995 and 2004 (Somi et at., 2006).
There is concern that a similar trend may not continue in Uganda where there is a decrease in consistent condom use and increase in the number of men with more than one partner (Uganda Ministry of Health, 2006). In addition, there is concern that the growing number of intravenous drug users, especially in Kenya, Tanzania, and Zanzibar may significantly modify the course of the epidemic in these regions (Ndetei, 2004; Odek-Ogunde, 2004).
West and Central Africa. The epidemic has been less severe overall in West Africa compared to East and Southern Africa. There is declining HIV prevalence in Ghana, Cote d’Ivoire, and Burkina Faso; however, prevalence appears to be increasing in Mali (WHO, 2005). In Mali, the HIV seroprevalence using antenatal clinic data has increased from 3.3% in 2002 to 4.1% in 2005. In Nigeria, which is known to have the third largest number of HIV-infected persons in the world, as a result of its large population, HIV prevalence appears to have stabilized at approximately 4.4% in 2005.
Asia: Overview. In 2006, there were 8.6 million people infected with HIV in Asia. Of these, 960 000 people were newly HIV- infected in 2006, and approximately 630 000 people died from AIDS. Compared to countries in sub-Saharan Africa, seroprevalence in most Asian countries is lower; however, generalized epidemics are found in Thailand, Cambodia, and Myanmar.
South-East Asia. South-East Asian countries have the highest HIV prevalence in Asia due to the commercial sex industry, widespread IDU, and transmission among men who have sex with men (MSM) (Figure 8). While the epidemic appears to be stabilizing in Thailand, Cambodia, and Myanmar, in Vietnam the number of infected individuals has almost doubled in number between 2000 and 2005. Despite the overall stabilizing trend in Thailand, there is a growing concern that the epidemic is increasing within the general population.
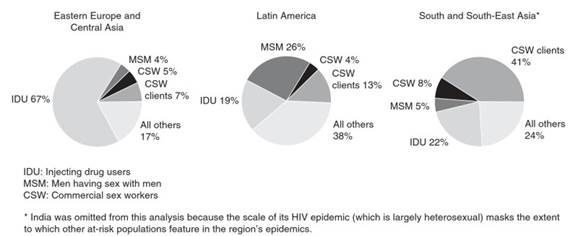
Figure 8. Proportions of HIV infections in different population groups by region, 2005. Reproduced with kind permission from UNAIDS/WHO (2007) AIDS Epidemic Update 2006. Geneva: UNAIDS/WHO
One-third of newly infected individuals in 2005 were married women. In Cambodia, the stabilizing trend may have been partly due to behavioral changes in the commercial sex work industry. Consistent condom use increased from 53% to 96% among brothel-based sex workers in the major cities of Cambodia (Gorbach et al, 2006) and this was followed by a decline in the HIV prevalence among sex workers from 43% to 21% between 1995 and 2003 (National Center for HIV/AIDS, 2004).
China. Currently, there are 650 000 people living with HIV in China, and approximately 45% of these individuals are intravenous drug users (China Ministry of Health, 2006). The epidemic initially occurred in rural provinces along the major drug trafficking routes, and major outbreaks from HIV-1 commercial plasma donors worsened the epidemic (Wu etal., 2001).
Sexual transmission has further fueled the spread of HIV to urban areas in China, which from 1998 to 2005 experienced an exponential increase in new HIV cases (Wu etal., 2007). New cases were estimated to climb from 3300 to 36 000 during this period, with a greater proportion due to sexual transmission in populations considered at lower risk. As a result, there is concern that the epidemic is now spreading from high-risk populations of intravenous drug users and commercial sex workers to the general population.
India. The second most populous nation, India, had approximately 5.7 million HIV-infected people in 2005, more than any other country in the world. Most of these reported HIV cases are concentrated in 6 of the 28 states of India where transmission is occurring through unprotected heterosexual intercourse. Among those infected, 38% are women and HIV prevalence among women from 206 antenatal clinics has declined from 1.7% in 2000 to 1.1% in 2004 (Kumar etal., 2006). The epidemics in the northeast part of India are mainly due to IDU.
Eastern Europe and Central Asia. Currently, there are 1.7 million people living with HIV in Eastern Europe and Central Asia, where new cases of HIV have grown significantly in the past decade and continue to increase. Ukraine and the Russian Federation comprise 90% of HIV infections of this region (EuroHIV, 2006), and approximately 80% of those infected in the Russian Federation are 15 to 30 years of age. The primary mode of transmission in this area is IDU, which makes up approximately 67% of cases in Eastern Europe and Central Asia (see Figure 8). However, the number of newly infected individuals through unprotected sex is also growing.
Latin America and the Caribbean. Approximately 250 000 people are living with HIV in the Caribbean. The epidemic was initially due to the commercial sex industry and eventually spread into the general population. In addition, 10% of those who are HIV-infected are MSM. The HIV infection rates have stabilized in the Caribbean, where Haiti and the Dominican Republic account for approximately 75% of HIV- infected cases.
In Latin America, the epidemic has stabilized overall with 1.7 million people living with HIV and approximately 140 000 new infections annually. The majority of the cases are due to unsafe IDU and MSM (see Figure 8), and more than 60% of HIV-infected persons reside in Argentina, Brazil, Colombia, and Mexico. There has been much international praise for the efforts of the Brazilian government for HIV prevention and treatment efforts during the last decade.
North America, Western, and Central Europe. In North America and Western and Central Europe, the number of living HIV-infected persons is 2.1 million, a number that continues to increase. The United States accounts for 1.2 million people living with HIV, which places it among the 10 countries in the world with the highest number living with HIV or AIDS. This is because individuals with HIV are living longer as a result of increased use of antiretroviral drugs in these parts of the world. In North America and Western and Central Europe, there were 65 000 new infections and approximately 30 000 deaths from AIDS in 2006.
The main populations at risk in the United States and Europe are MSM and intravenous drug users. However, women, African-Americans, and immigrants are increasingly affected by the HIV epidemic. The proportion of women newly infected with HIV increased from 15% before 1995 to 27% in 2004 in the United States, and between 2001 and 2004, half of all AIDS diagnoses were in African-Americans. In 2004, African-Americans had a significantly higher risk of HIV infection than among Whites in the United States, 7 times greater in men and 21 times greater in women. In Western and Central Europe, three-quarters of all heterosexually acquired HIV are among migrants and immigrants (EuroHIV, 2006).
Middle and North Africa. There are an estimated 450 000 people living with HIV, with 68 000 newly infected, in Middle and North Africa. The major modes of transmission are IDU, commercial sex, and sex among MSM. In this region, Sudan is the only nation with a generalized epidemic with a prevalence of 1.6%. Other nations in this region have poor surveillance, and therefore it may be difficult to understand fully the nature of the epidemic. Greater efforts are needed to improve surveillance and access to high-risk populations to control the HIV epidemic.
Oceania. In Oceania, an estimated 81 000 persons were infected with HIV and 7100 were newly infected in 2006. Three- quarters of the infected in this region reside in Papua New Guinea, where prevalence has increased to 1.8%. Risk factors for transmission in Papua New Guinea include inconsistent condom use, sex with commercial sex workers, high rates of concurrent sexual relationships, early sexual initiation, high rates of sexual violence against women, and high rates of STIs (Brouwer et al, 1998; Bank, 2006). In Australia and New Zealand, transmission among MSM continues to drive the epidemic, accounting for 66% and 90% of all new HIV cases, respectively.
See also: AIDS: Overview; HIV Safety Guidelines.
Citations: Abbott RC, NDour-SarrA, Diouf A, et al. (1994) Risk factors for HIV-1 and HIV-2 infection in pregnant women in Dakar, Senegal. Journal of Acquired Immune Deficiency Syndromes 7: 711-717.
Adjorlolo-Johnson G, De Cock KM, Ekpini E, etal. (1994) Prospective comparison of mother-to-child transmission of HIV-1 and HIV-2 in Abidjan, Ivory Coast. Journal of the American Medical Association 272: 462-466.
Alaeus A, Lidman K, Bjorkman A, Giesecke J, and Albert J (1999) Similar rate of disease progression among individuals infected with HIV-1 genetic subtypes A-D. AIDS 13: 901-907.
Amato L, Minozzi S, Davoli M, Vecchi S, Ferri M, and Mayet S (2004) Psychosocial combined with agonist maintenance treatments versus agonist maintenance treatments alone for treatment of opioid dependence. Cochrane Database of Systematic Reviews 4, CD004147.
Andreasson PA, Dias F, Naucler A, Andersson S, and Biberfeld G (1993) A prospective study of vertical transmission of HIV-2 in Bissau, Guinea-Bissau. AIDS 7: 989-993.
Anthony JC, Vlahov D, Nelson KE, Cohn S, Astemborski J, and Solomon L (1991) New evidence on intravenous cocaine use and the risk of infection with human immunodeficiency virus type 1. American Journal of Epidemiology 134: 1175-1189.
Asian Development Bank (2006) www.adb.org/Documents/RRPs/ PNG/39033-PNG-RRP.pdf (accessed April 2008).
Astemborski J, Vlahov D, Warren D, Solomon L, and Nelson KE (1994) The trading of sex for drugs or money and HIV seropositivity among female intravenous drug users. American Journal of Public Health 84: 382-387.
Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, and Puren A (2005) Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: The ANRS 1265 Trial. Public Library of Science Medicine 2: e298.
Baeten JM, Chohan B, Lavreys L, etal. (2007) HIV-1 Subtype D Infection Is Associated with Faster Disease Progression than Subtype A in Spite of Similar Plasma HIV-1 Loads. Journal of Infectious Diseases 195: 1177-1180.
Baeten JM and Overbaugh J (2003) Measuring the infectiousness of persons with HIV-1: opportunities for preventing sexual HIV-1 transmission. Current HIV Research 1: 69-86.
Bailey RC, Moses S, Parker CB, etal. (2007) Male circumcision for HIVprevention in young men in Kisumu, Kenya: a randomised controlled trial. The Lancet 369: 643-656.
Barin F, M'Boup S, Denis F, et al. (1985) Serological evidence for virus related to simian T-lymphotropic retrovirus III in residents of west Africa. The Lancet 2: 1387-1389.
Bell DM (1997) Occupational risk of human immunodeficiency virus infection in healthcare workers: an overview. American Journal of Medicine 102: 9-15.
Biggar RJ, TahaTE, Hoover DR, Yellin F, Kumwenda N, and Broadhead R (2006) Higher in utero and perinatal HIV infection risk in girls than boys. Journal of Acquired Immune Deficiency Syndrome 41: 509-513.
Relevant Websites: http://www.aidsinfo.nih.gov - AIDSinfo, HIV/AIDS Treatment Information, Department of Human and Health Services Guidelines.
http://www.cdc.gov - Centers for Disease Control and Prevention (CDC).
http://www.hivma.org/Content.aspx?id=1922 - HIV Medicine Association (HIVMA) Practice Guidelines.
http://www.unaids.org - Joint United Nations Programme on HIV/AIDS (UNAIDS).
http://www.iasusa.org/pub/arv_2006.pdf - Treatment for Adult HIV Infection: 2006 Recommendations of the International AIDS Society - USA Panel.
Date added: 2024-02-18; views: 635;