AIDS, Epidemiology and Surveillance
Introduction. During the last 25 years, human immunodeficiency virus (HIV) has claimed the lives of millions of men, women, and children across the globe and has developed into an international public health crisis. The HIV/AIDS (acquired immune deficiency syndrome) epidemic has spared few regions in the world and has been particularly devastating in sub-Saharan Africa, where more than 60% of all HIV- infected adults and 90% of HIV-infected infants reside (Joint United Nations Program on AIDS [UNAIDS]/World Health Organization [WHO], 2006).
At the time of the first reports of AIDS cases among gay men in the United States during the early 1980s, it would have been difficult to envision such a calamitous outcome. Even after identification of the human immunodeficiency virus in 1983 and diagnosis of HIV infection among heterosexual men and women, infants and children, intravenous drug users, hemophiliacs, and recipients of other blood products, the enormity of the situation was not fully recognized.
As a result, the global response to HIV was initially slow and in many parts of the world remains inadequate, despite in-depth knowledge of the salient risk factors for HIV transmission and improved surveillance data defining the nature of the epidemic.
Overall Prevalence of HIV. Despite significant advances in HIV prevention and treatment, HIV remains a disease without a cure and continues to threaten the social and economic stability of many developing nations. According to the AIDS Epidemic Update 2006 by UNAIDS, an estimated 39.5 million (34.1-47.1) people worldwide were living with HIV in 2006 (Figure 1).
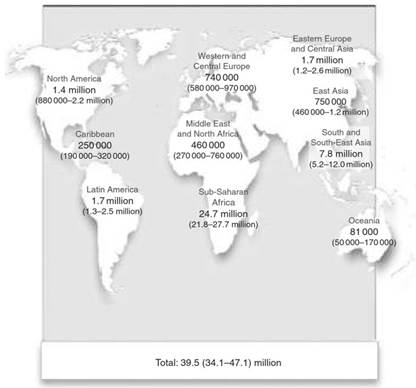
Figure 1. Adults and children estimated to be living with HIV in 2006. Reproduced with kind permission from UNAIDS/WHO (2007) AIDS Epidemic Update 2006. Geneva: UNAIDS/WHO
Approximately 17.7 million (15.1-20.9) of HIV-infected were women, an increase of over 1 million between 2004 and 2006. In the same year, an estimated 4.3 million (3.6-6.6) became newly infected with HIV, and approximately 2.9 million (2.5-3.5) lost their lives to AIDS (Figures 2 and 3). HIV has infected over 65 million people and claimed over 25 million lives worldwide since 1981 (UNAIDS/ WHO, 2006).
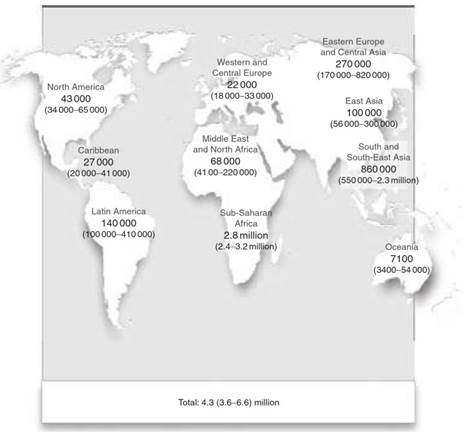
Figure 2. Estimated number of adults and children newly infected with HIV during 2006. Reproduced with kind permission from UNAIDS/WHO (2007) AIDS Epidemic Update 2006. Geneva: UNAIDS/WHO
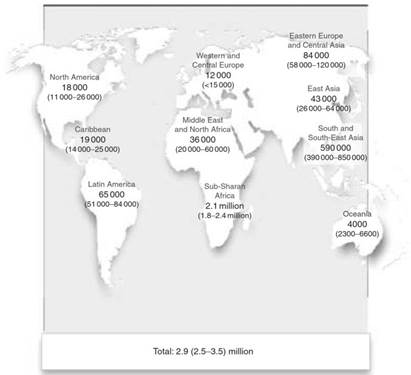
Figure 3. Estimated adult and child deaths from AIDS during 2006. Reproduced with kind permission from UNAIDS/WHO (2007) AIDS Epidemic Update 2006. Geneva: UNAIDS/WHO
Distinctions between HIV Types 1 and 2. Two human immunodeficiency viruses have been identified and characterized in humans: HIV type 1 (HIV-1) and HIV type 2 (HIV-2). While HIV-1 and HIV-2 share the same modes of transmission, HIV-2 has a less efficient rate of transmission than HIV-1 (Kanki et al, 1994). Studies conducted in Senegal estimated the HIV-2 transmission rate per sexual act with an infected partner to be 3.4- to 3.9-fold lower than that of HIV-1 (Gilbert et al., 2003).
Other studies conducted in The Gambia, Ivory Coast, and Senegal have demonstrated rates of mother-to-child HIV-2 transmission to be approximately 6- to 20-fold lower than those among women with HIV-1 infection (Andreasson etal., 1993; Abbott et al., 1994; Adjorlolo-Johnson etal., 1994; O’Donovan et al., 2000). Studies have also demonstrated that progression to AIDS is slower among individuals with HIV-2 compared to HIV-1, although the consequences of immunosuppression and the propensity for opportunistic infections remain similar at lower CD4 counts (Marlink etal, 1994).
Another difference between HIV-1 and HIV-2 is in their antiretroviral susceptibility, which may be important in future delivery of antiretroviral therapy to Africa and management of the epidemic. The current antiretroviral therapy for HIV-1 includes various combinations of nucleotide or nucleoside reverse transcriptase inhibitors (NRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), and protease inhibitors (PIs). While NRTIs have been found to be as effective against HIV-2 as they are against HIV-1 in vitro (Mullins et al, 2004), NNRTIs have been shown to be largely ineffective against HIV-2 in vitro (Witvrouw et al, 1999). PIs have shown mixed effectiveness against HIV-2 (Pichova etal., 1997).
Given lower rates of transmission and progression to disease with HIV-2, it is not surprising that HIV-1 is responsible for the majority of HIV infections and AIDS cases worldwide. HIV-2 is restricted to relatively small geographic areas and is the predominant HIV type in the West African countries of Guinea-Bissau, The Gambia, Cape Verde, and Senegal, where it was first described in 1985 (Figure 4) (Barin et al, 1985). HIV-2 is also found in Portugal and former Portuguese colonies, such as Mozambique, Angola, southwestern India, and Brazil, although it is less prevalent in these regions than HIV-1 infection (Kanki, 1997).
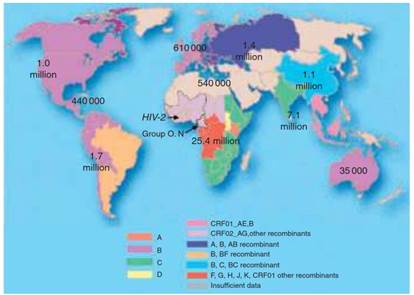
Figure 4. Global distribution of HIV-1 subtypes and HIV-2. Global epidemiology of HIV 78: s7–s12. Copyright 2006 Wiley & Sons, Inc. Reprinted with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc.
While these differences between HIV-1 and HIV-2 promote a better understanding of HIV, it is clear that HIV-1 drives the HIV/AIDS epidemic globally, and HIV-1 will therefore be the focus of the remainder of this article.
HIV-1 Groups and Subtypes. The great genetic diversity of HIV is reflected in the many genotypes or clades that have been identified. Currently, HIV-1 genotypes are divided into Groups M, N, and O, with Group M being further subdivided into subtypes A to K because it is the most common. Groups N and O are limited to West Africa. Group O represents the outlier strains, while Group N represents ‘new group’ or non-O and non-M strains. Generally, intragenotype strain variation is less than 15%, while intergenotypic variation is 20-30% (Burke, 1997).
Subtypes A to K are defined by significant clustering across the genome and are often more prevalent in particular regions of the world (see Figure 4) (McCutchan, 2006). Of these subtypes, subtype C is currently the most common subtype worldwide, and is found in the eastern and southern parts of Africa and in India (McCutchan, 2000). Subtype B predominates in the United States and Europe, subtypes A and D are found in eastern parts of Africa, and subtype E in South-East Asia.
Several studies suggest that subtypes A to K differ in their primary mode of transmission, virulence, and infec- tivity. In Thailand, where subtypes B and E were both prevalent at the start of the epidemic, subtype E was initially the major subtype among female sex workers, while subtype B was associated with intravenous drug use (IDU) (Nelson et al., 1993; Nopkesorn et al, 1993). However, subtype E subsequently became more common than subtype B among IDUs, indicating that mode of transmission may be less important than other biological or behavioral factors (Nopkesorn et al., 1993).
In Kenya, subtypes A, C, and D all circulate and individuals infected with HIV-1 subtype C have been found to have higher plasma RNA levels and lower CD4 counts compared to individuals with subtypes A or D (Neilson et al., 1999). In Uganda and Kenya, HIV infection with subtype D has been associated with more rapid progression when compared to infection with subtype A (Kaleebu et al., 2001; Baeten et al., 2007). However, in Sweden, studies showed no differences among subtypes A, B, C, or D when examining clinical HIV disease progression (Alaeus etal., 1999).
Individuals may also be coinfected with 2 strains of HIV-1 and these may be the same or different viral subtypes. Coinfection occurs when a person acquires two different viral strains simultaneously or when a chronically HIV-infected individual is reinfected with HIV-1, a phenomenon also known as super-infection. This has led to recombinant forms of HIV-1, which may in turn be transmitted and have the potential to become major strains within populations.
For example, a recombinant form comprised of subtypes A and E is a major circulating strain throughout South-East Asia and a recombinant strain of subtypes A and G is a major strain in West Africa. Recombinant strains will undoubtedly continue to emerge and challenge those involved in HIV vaccine development, surveillance efforts, and clinical care.
Date added: 2024-02-18; views: 662;