Interventions to Reduce Induced Abortions
Abortions are the result of unwanted pregnancies; therefore, the logical strategy for decreasing the number of abortions is to help women avoid unwanted pregnancy. However, even after an unwanted pregnancy has occurred, the number of abortions can be reduced by providing the pregnant woman with the social support she needs to have a baby without sacrificing her plans for the future.
Prevention ofunwanted pregnancy has proven to be the most effective strategy for decreasing the number of abortions. The low abortion rate in Western Europe coincides with conditions that favor the prevention of unwanted pregnancies. The high incidence of abortion in Latin America and Eastern Europe is a result of limited access to effective means for preventing unwanted pregnancy.
Family Planning. The 1994 International Conference on Population and Development (ICPD) Programme of Action urged all governments to “strengthen their commitment to women’s health’’ and ‘‘deal with the health impact of unsafe abortion as a major public health concern.’’ The conference participants pledged their commitment to reducing the need for abortion ‘‘through expanded and improved family planning services.’’
The call to reduce abortion through family planning is based on the global experience acquired over the decades since modern hormonal contraceptives and IUDs became widely available. In 1966, the Chilean Government established family planning as an official component of the women’s health-care program, providing free contraceptive services to 85% of the population through the National Health Service.
Several authors confirmed a direct correlation between improved access to contraceptives and the dramatic decrease in the number of women with abortion complications who were admitted to public hospitals; these data are illustrated in Figure 3. Similarly, in Brazil, the number of abortion complications dealt with by the national health service dropped from approximately 345 000 in 1992 to 228 000 in 1998 after the rapid increase in the use of modern contraceptives.
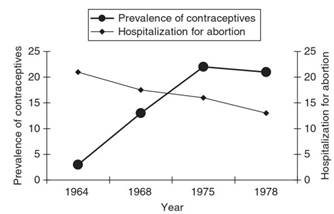
Figure 3. Prevalence of contraceptives (Statistical Service) and proportion of abortions related to all hospitalizations. Chile, 1964-78. Adapted from Maine D (1981) Family Planning: Its Impact on the Health of Women and Children. New York: Columbia University Center for Population and Family Health
Experience from many countries shows that when there is a rapid decrease in desired family size, contraceptive use increases, but induced abortions may also increase iffamily planning access cannot satisfy the increased demand. Only when the unmet need for contraception has been met does the number of induced abortions invariably decline.
Sex Education. The majority of studies have shown that sex education programs of adequate duration, content, and methodology are effective in reducing pregnancy and abortion. Programs with greater effectiveness are those that promote responsibility, abstinence, and (for those who are sexually active) protection against pregnancy and sexually transmitted infections.
Successful programs combine the promotion of mutual respect and gender power balance with knowledge of sexual and reproductive physiology and sexually transmitted infection, knowledge that is mostly lacking, particularly among young people in developing countries.
Contrary to the fears of some people, sex education does not increase sexual activity or promote early sexual experimentation; on the contrary, it may encourage adolescents to postpone the initiation of sexual activity, thus reducing the proportion of adolescents who have sexual relations.
The countries with the lowest abortion rates are those that have broad-based, progressive sex education programs in their schools and nearly universal school attendance. The Netherlands and several European Nordic countries fulfilling these conditions have the lowest teen abortion and teen pregnancy rates. This has been achieved through implementation of comprehensive sex education; confidential, high-quality family planning services; and access to a wide selection of contraceptive methods.
Age of first intercourse has remained unchanged in these countries, but contraceptive use has increased dramatically. For instance, a study in Finland showed that in 1997, 87% of sexually active 16-year-old girls had used a condom during their last intercourse. These data suggest that sex education is an effective intervention for reducing gender power imbalance and promoting mutual respect concerning sexual decisions, a basic factor in the efforts to reduce unwanted pregnancy and abortion.
In contrast, countries that have a high abortion rate either have no sex education programs or have local programs that are narrow in scope. The emergency created by the HIV epidemic has stimulated the acceptance of sex education, but the lack of both adequately trained personnel and strong political support reduces the effectiveness of the few programs that are being implemented.
Other Interventions. Young, unmarried women may become pregnant as a result of a subconscious or conscious desire to have a child. They may be pleased to be pregnant in the expectation that, with the support of a partner or family, their motherhood will not interfere with continuing their education or career.
Since their partners may disappear when they learn of the pregnancy and family support may be lacking, these women end up choosing pregnancy termination as the only viable alternative. Studies show that women who find themselves in this situation might have continued their pregnancies if they had received more support.
Support is needed not only from the family but also from society as a whole. Society must ensure, for instance, that a pregnant adolescent does not have to interrupt her studies in order to have a baby if she wishes to do so. Otherwise, she will have to decide between having a baby but discontinuing her studies or aborting as the only means of achieving her objectives for the future.
An adult pregnant woman needs support to keep her job, needs to receive appropriate care during pregnancy, delivery, and the postpartum period, and facilities enabling her to continue her career while breastfeeding and taking care of her baby. Without that support, she may have to decide between aborting and losing a job that is incompatible with pregnancy, delivery, breastfeeding, and child care.
Date added: 2024-02-03; views: 741;