Tomography in Medicine. First Generation Computed Tomography (CT)
The word tomography derives from the Greek word tomos meaning a section, and the technique was proposed by Gustave Grossman in papers published in 1935 describing the experimental details of tomography and its clinical application.
A tomographic image is essentially a picture of a slice of the patient’s anatomy. Developments in x- ray tomography culminated at the end of the twentieth century with the invention of computed tomography (CT), which has found numerous applications in diagnostic medicine including scanning for cancer, subdural hematomas, ruptured disks and aneurysms. It substantially reduced the requirement for exploratory surgery.
Tomographic techniques are also employed in other diagnostic imaging modalities such as ultrasonography. Early B-Mode ultrasound scanners were mounted a single transducer element on an articulated arm to produce an acoustic tomographic slice of the body. The arm was moved through a series of positions to allow the ‘‘slice’’ of data to be collected.
In standard x-ray imaging, three-dimensional patient information is projected onto a twodimensional surface. Each point on the image is a projection of the attenuating properties of all the tissues along the x-ray beam’s path. Tomographic techniques sought to examine a section through the body ignoring the tissue above and below the section of interest.
In early x-ray tomography, the x-ray tube traveled in an arc above the patient while the film cassette in the table, beneath the patient, traveled in the opposite direction so that x-rays remain incident on the film throughout the exposure (Figure 9).
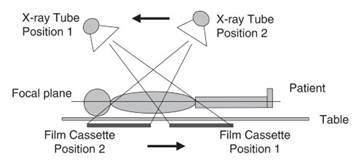
Figure 9. Motion of the x-ray tube and film cassette in x-ray tomography
The patient was positioned so that the area of interest within the body was at the focal plane of the x-ray tube. When the x-ray tube moved through the tomographic angle, objects above and below the focal plane were blurred, thereby largely obliterating their contrast.
As a result, the objects at the focal plane were seen more clearly than objects above and below the plane. The tomographic angle determines the slice (depth of objects in the focal plane) thickness. As the out- of-plane anatomy is not removed from the image, but blurred out, the effective image contrast is reduced. The clinical importance of tomography was quickly established, and the first atlas of clinical tomograms was compiled in 1940.
The development of CT followed from the work of numerous scientists who had built a variety of apparatus that aimed at true section imaging, which is achieved when the presence of planes above and below the image are of no consequence. Gabriel Frank (1940) showed how a transverse axial section can be sharply imaged without contribution from adjacent sections. Images were reconstructed by a form of optical back-projection, a method that emulates the image acquisition sequence in reverse.
This was a form of CT without the computing, three decades before CT was developed. A Japanese radiologist, Shinji Takahashi, conducted a series of experiments in the 1940s and 1950s which also anticipated the later developments in CT. W.H. Oldendorf (1961) designed an apparatus to measure radiodensity at a point, uncoupling the effects of all other points in the same plane. This was achieved by arranging that the signals were at different frequencies. Oldendorf is often credited with producing the first laboratory CT of a ‘‘head’’ phantom.
Development of emission tomography methods overlapped with the development of transmission CT. Tomographic nuclear medicine was studied in the 1960s and developed into computerized tomography with the invention of single photon emission computed tomography (SPECT) in the 1970s. Experimental work leading to the development of modern positron emission tomography (PET) systems began in the 1950s.
In 1972 Godfrey Hounsfield, a British engineer employed by Electric and Musical Industries (EMI), developed the first CT system. CT technology quickly evolved through a series of generations with most of the initial developments focusing on increasing the scanning speed and thus reducing problems with patient motion.
Developments in computing complemented these advances enabling rapid reconstruction of images from the huge data sets obtained. Hounsfield’s scanners included what have become known as first, second, and third generation scanners developed between 1972 and 1977. Although numerous designs of scanners were patented (particularly in later generation scanners) the following broadly applies to the designs.
First generation systems used an x-ray tube, which emitted pencil beam x-rays. Transmitted x- rays were measured by a single detector (per slice). The tube and detector were translated across the object to acquire x-ray transmission data (Figure 10). The detector and x-ray tube were then tilted at an angle of 1 degree, and the translation process was repeated until the system had completed a 180- degree rotation and a complete set of CT data was obtained. Approximately 30,000 projections were taken with scanning times running to several minutes per slice.
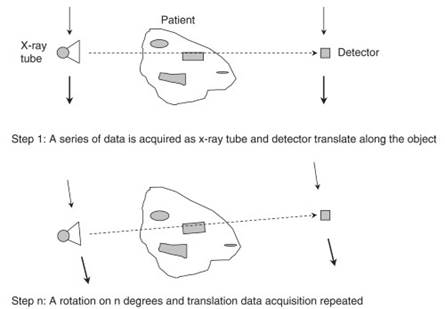
Figure 10. First generation computed tomography (CT)
Second generation CT scanners employed a linear array of 30 detectors to collect x-ray transmission data. The x-ray beam was collimated to a narrow fan. Second generation scanners did not have as good scatter rejection as first generation but slice acquisition time was as much as 15 times faster. Additional data detection capability was used to increase speed of acquisition and image quality.
By the mid-1970s third generation scanners had been developed, and these were the first fast medical scanners. More than 800 detectors were employed, arranged in an arc encompassing the width of the patient. This eliminated the need for translation motion. In this design both tube and detectors rotate together inside a gantry to acquire the necessary projections. Scan times per slice were reduced to approximately 5 seconds.
In the late 1970s, fourth generation CT scanners were built with approximately 5000 individual detectors arranged in a 360-degree ring around the patient (Figure 11). The detectors remain stationary while the tube is rotated.
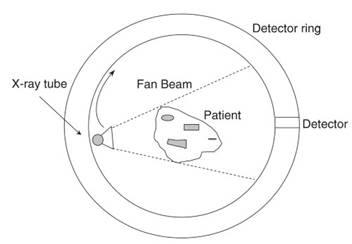
Figure 11. Fourth generation scanner. The detectors are fixed in a ring around the patient, and the x-ray tube rotates during acquisition
Obtaining CT images requires taking x-ray transmission measurements at numerous angles around the object. This is roughly analogous to precisely locating the seeds inside an orange by probing it from many points with a thin wire. The image may be built up through a back-projection technique, which is essentially a mathematical method for establishing the geometry of the object based on data collected from x-rays taken at multiple angles through the object.
The mathematical principles underlying CT were developed by an Austrian mathematician, Johann Radon, in 1917. Radon theoretically demonstrated that an image of an unknown object could be reproduced from an infinite number of projections through the object. Images are reconstructed from the raw data through sophisticated algorithms. This involves processing 800,000 or so projections for each picture element (pixel) displayed, as well as applying image-processing algorithms.
Filtered back projection is a common algorithmic image reconstruction technique. The process emulates the acquisition procedure in reverse and convolves the solution with a filter of kernel to correct for known errors in the reconstruction process and to emphasize particular characteristics in the image. Different kernels are available for types of soft tissue and bone and may be selected by the operator.
Digital technology for display of images became prominent in the 1980s. Image displays for CT typically have a 512 by 512 display matrix with each pixel in the matrix having a distinct value (or CT number) based on the calculated attenuation value for the corresponding volume element (or voxel) in the patient. Images are usually presented as a series of two-dimensional images on a monitor, with each image representing a slice through the patient. Computer programs can also produce three-dimensional reconstruction of CT images.
The development of CT has been compared in significance to Wilhelm Roentgen’s discovery of x- rays. Hounsfield won the Nobel Prize for Medicine rather than Physics, reflecting the considerable clinical benefits in producing high-contrast images of slices through a patient. Developments in CT technology through the 1980s included the helical CT scanners that acquire information while the table moves the patient through the ring of detectors.
The effect of this linear translation through a rotating acquisition is to produce a helical or spiral motion of the x-ray tube around the patient. Helical scanners increase the efficiency of multislice acquisition and reduce overall scanning time.
The 1990s saw the development of multidetector arrays. In these systems slice width is determined by the way the detectors are grouped together rather than by beam collimation, as was the case in earlier generations. Multidetector arrays bring CT imaging systems closer to acquiring a full threedimensional data set by reducing slice thickness to about 0.5 millimeters.
Date added: 2023-10-26; views: 906;