To Which Disease and Injury Conditions is Alcohol Causally Relevant?
Two general types of disease and injury conditions causally impacted by alcohol can be distinguished (Rehm et al., 2003a): (1) disease and injury conditions that are caused by alcohol by definition (e.g., alcohol dependence or alcohol intoxication), and (2) disease and injury conditions in which alcohol is a contributory cause. In identifying the latter (current burden of disease study), the usual epidemiological standards were applied.
Thus, to establish sufficient evidence of causality there had to be: (1) consistent evidence of an association (positive or negative) between alcohol consumption and the disease or injury; (2) chance, confounding variables, and other bias could be ruled out with reasonable confidence as factors in this association; and (3) evidence of a plausible mediating process (English et al, 1995). These judgments were made using the usual criteria for establishing causality in epidemiology, with the most weight placed on the following four criteria:
1. Consistency across studies;
2. Established experimental biological evidence of mediating processes or at least physiological plausibility (biological mechanisms);
3. Strength of the association (effect size); and
4. Temporality (i.e., cause before effect).
Disease and injury conditions wholly attributable to alcohol. With regard to the attribution of alcohol-relatedness, the conditions shown in Table 1 are, by definition, wholly attributable to alcohol and thus have an alcohol-attributable fraction of 100% (AAF; see under ‘Risk relations’ for equation). In other words, in a counterfactual scenario of no presence of alcohol, these disease conditions would not exist. For these conditions, no statistical procedures are necessary to estimate risk relationships.

Table 1. Disease and injury conditions that are by definition alcohol related (AAF = 1 or 100%)
This does not mean that the underlying data are always free of measurement error, that is, that all diagnoses of ‘alcoholic cirrhosis of liver’ are caused by alcohol. Measurement error may also work in the opposite direction, for example, alcoholic liver cirrhoses are not identified as such and erroneously classified as other forms of liver cirrhosis.
Chronic disease conditions and injuries in which alcohol is a contributory cause. Table 2 gives an overview of chronic conditions that are not wholly attributable to alcohol, but in which alcohol has been identified as causally relevant, based on the previously mentioned four criteria. Two examples of the considerations undertaken with regard to somewhat controversial outcomes illustrate this process. For lung cancer, after adjusting for smoking, meta-analyses showed a clear relationship.
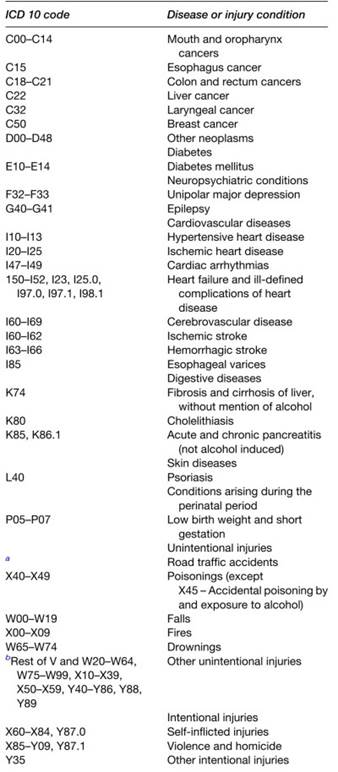
Table 2. Disease and injury conditions that are not by definition wholly attributable to alcohol (AAF < 1)
However, since evidence for the possible biological mechanism was not conclusive and residual confounding from smoking could not be excluded, English and colleagues (1995), in their first seminal assessment, decided to exclude lung cancer from the list of diseases causally influenced by alcohol. A decade later, we still believe this judgment is correct, although some tentative pathways have meanwhile been established.
In contrast, although English et al. (1995) concluded there was not sufficient evidence linking alcohol consumption and breast cancer, recent advances both in biological and epidemiological research have changed this evaluation, so that breast cancer was included in this article as an alcohol-related outcome. Similar scientific advances hold true for colorectal cancer. These two conditions were the only two that had been added to the list in the last decade.
Date added: 2024-03-11; views: 714;