Apical and Periodontal Radiographic Technique
Special radiographic techniques are necessary to show the apical and periodontal structures adequately, for two reasons:
- The best resolution as well as the least distortion will appear on the radiograph at the area where the central ray traverses the tissue.
- Only those tissues that have been exposed appropriately with regard to their thickness and density will be optimally depicted in the radiograph.
For these reasons, in order to produce a high-quality apical or periodontal radiograph, the central ray must pass through either the root apex or the alveolar crest. The exposure data must be selected corresponding either to the thickness of the bone at the level of the root apices or for proper depiction of the thinner alveolar crest. Taken to extremes, this means that if perfect depiction of the apical region is desired, the depiction of the tooth crown and the alveolar crest must be sacrificed to some degree; on the other hand, for a perfect periodontal projection, the depiction of the root apex will be compromised.
In reality, of course, nobody who is preparing a conventional radiographic survey will be prepared to consciously renounce the simultaneous depiction of the tooth crown and the root apex! However, since the introduction of the panoramic radiograph as the basic diagnostic film, new ideas concerning targeted application for the periapical radiograph have begun to evolve. On the other hand, because the concept of a more modern examination strategy using panoramic radiography does not yet enjoy general acceptance, a compromise must be found.
One realistic approach to improve the still often used conventional radiographic survey is the regular use of a film holder that guarantees optimum positioning. In this regard, systems that position the film at a right angle to the X-ray tube have proved themselves in clinical practice; in this way, the separate, tiresome, and “free-hand” positioning of the film and the X-ray tube can be replaced by a compact targeting mechanism that virtually guarantees accuracy. In addition to improving conventional radiographic technique, film quality is improved and radiation dose is reduced.
Numerous investigators today are reporting new diagnostic possibilities offered by subtraction radiography and radiovisiography. These represent new and promising technologies. However, they must now satisfactorily pass a sufficient period of testing before they can be recommended for the daily practice.
As already mentioned, exposure data must be selected on the basis of the question to be answered. For the diagnosis of apical problems, the exposure data must be appropriate for the thickness of the bone surrounding the apex. If possible periodontal involvement is to be examined, the exposure data must be selected in appropriate relation to the thickness of the interdentally visible alveolar crest.
Radiographic Surveys for Patients of Various Ages. Depending upon the diagnostic questions that are encountered during the individual phases of growth and in patients of various ages, several different types of intraoral radiographic surveys may be indicated. Since the space available for the intraoral positioning of films varies considerably depending upon the age of the patient, various film formats have been developed to satisfy the diagnostic demands.
The film formats that have been developed over the course of the past decades based on clinical experience should be standardized as much as possible rather than being altered at the user’s discretion. To ensure a high quality radiograph and to avoid unnecessary radiation exposure by retakes, each radiographic technique must be perfected through standardization. With the regular use of an appropriate film holder, one can avoid the numerous sources of error that accompany “free-handed” positioning of the film and the X-ray tube.
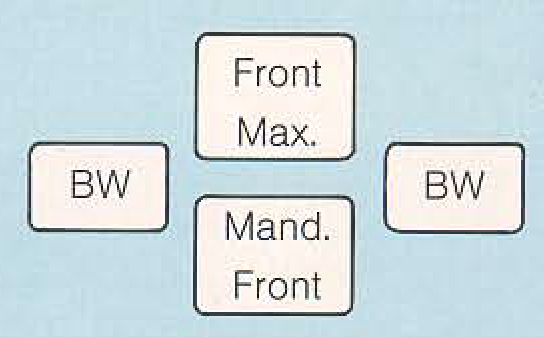
Radiographic survey for preschool children. This survey consists of two periapical radiographs (middle) and two small bite-wing radiographs using film size 2x3 cm. The periapical films are positioned as occlusal projections.
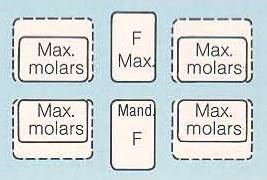
Radiographic survey for 6-year-old children. This radiographic survey for smaller children consists of 2 x 3 cm films or, for larger children two 2 x 3 cm films and four 3 x 4 cm films (dashed outline).
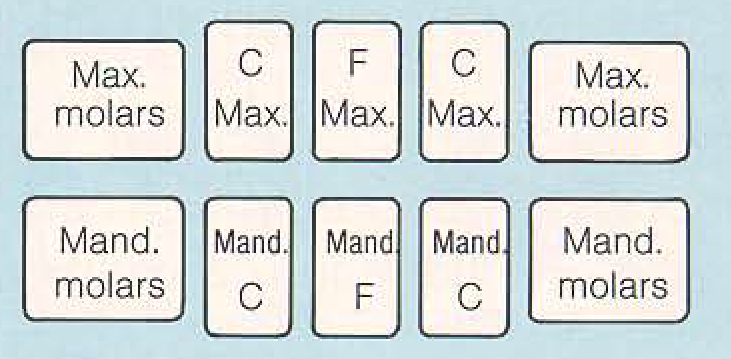
101. Radiographic survey for children with mixed dentition. Six narrow child films are used to depict incisor (F) and canine (C) regions. Premolars and first permanent molars can be captured using periapical films.
Radiographic survey for children nearing the end of the mixed dentition stage. The previously described 10-film survey (Fig. 101) is expanded by the addition of one more film in each molar region. This survey is also well indicated for use in adults with a narrow anterior arch.
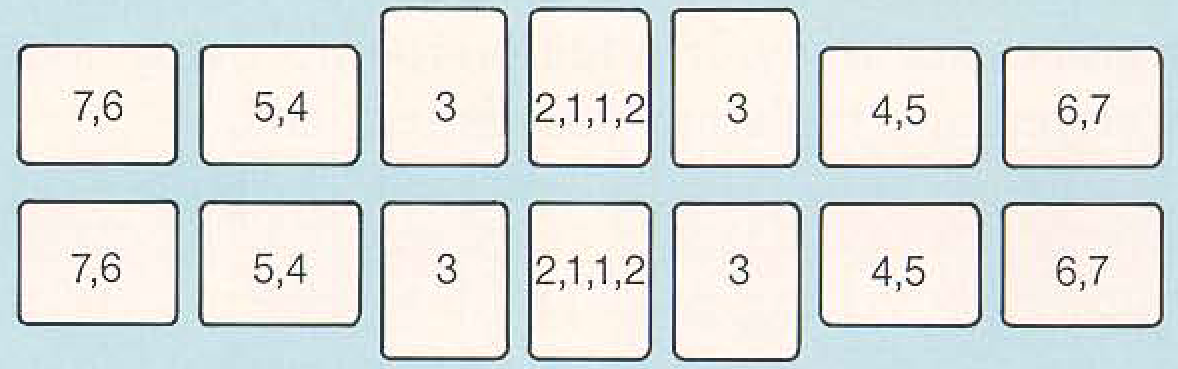
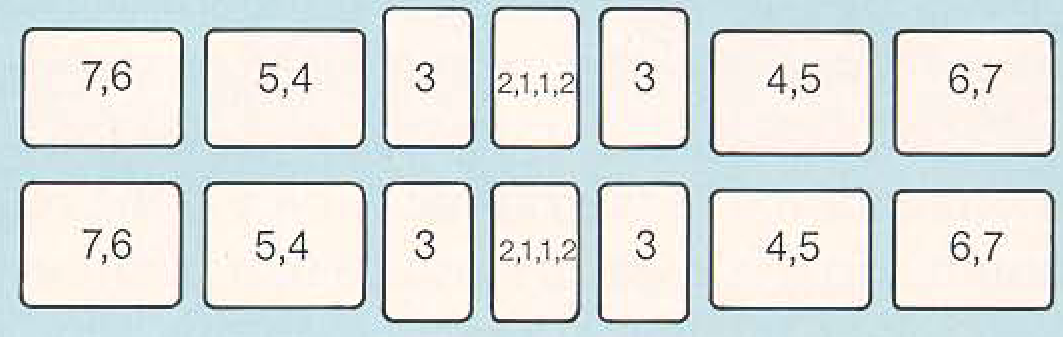
Typical 14-film survey for adults. This survey will encompass all but the third molars, whose shapes and positions are extremely variable. Special radiographic techniques must be used sometimes for appropriate depiction of third molars.
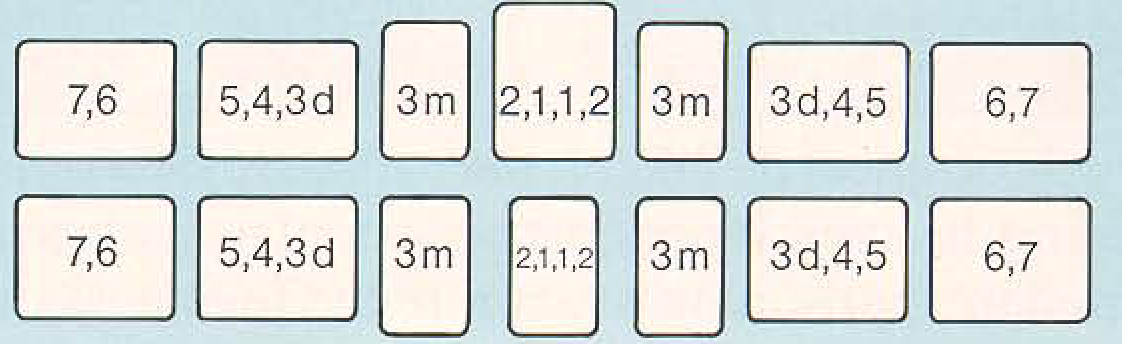
Reduced periodontal radiographic survey using 14 films. The normal 18-film periodontal survey can be reduced to a 14-film series if the right-angle system from Beycodent is employed as described by Pasler.
Date added: 2022-12-17; views: 799;