The Bite-Wing Radiograph. Examples
The bite-wing radiograph is without doubt the most important supplemental film for data collection in addition to the panoramic film. Even though, thanks to modern preventive dentistry, the prevalence of dental caries has been dramatically reduced, early diagnosis of caries using the bite-wing radiograph continues to be of central importance for the early detection of incipient proximal caries.
Clinical experience shows, of course, that radiographic examination for fissure caries is helpful only in late stages of lesion development, while buccal and lingual or palatal lesions are hardly ever seen on radiographs; in these cases, careful clinical inspection plays the most important role. The reason for this fact can be explained by the mechanism of action of X-rays; only those tooth surfaces that are not superimposed by dense, healthy tooth substance and that are struck tangentially by the central ray will appear as radiolucencies, thus signaling incipient loss of hard tooth structure. Tooth surfaces (Class V) that are perpendicular to the central ray or which are superimposed by the entire thickness of an intact crown, e.g., fissure caries, elicit no radiographic sign of early carious lesions.
On the other hand, because it functions according to the principles of tomography, panoramic radiography can reveal loss of tooth substance with surprising clarity if taken with precise positioning. This should not, however, be taken as a reason to disregard the bite-wing radiograph when it comes to checking for proximal caries.
In summary, the bite-wing radiograph can provide the following information:
- Early diagnosis especially of proximal caries
- Checking the marginal closure of restorations and crowns in the proximal area
- Evidence of existing endodontic treatments in the posterior segments
- Documentation of calculus accumulation in the proximal spaces of posterior teeth
- Condition of the alveolar ridge in the posterior region, if the projection relationships are ideal
- Existence of malocclusion in the posterior region caused by missing teeth, missing antagonists or premature contacts
Good radiographic depiction of caries and malocclusion requires a higher energy exposure, while the depiction of restoration margins as well as cervical and periodontal problems require lower energy. Depending upon the age of the patient, various sizes of bite-wing films are available. The dentition from the distal surface of the canine to beyond the second molars should be captured on the bite-wing radiograph.
In order to display the alveolar ridge as completely as possible, the elevation must be optimum, which necessitates using only those film holders with bite tabs no thicker than paper. Used in this way the bite-wing radiograph and the panoramic film not only provide the basis for data collection but also serve as an excellent radiographic survey for the regular evaluation of the condition of the posterior teeth, while providing minimum radiation exposure.
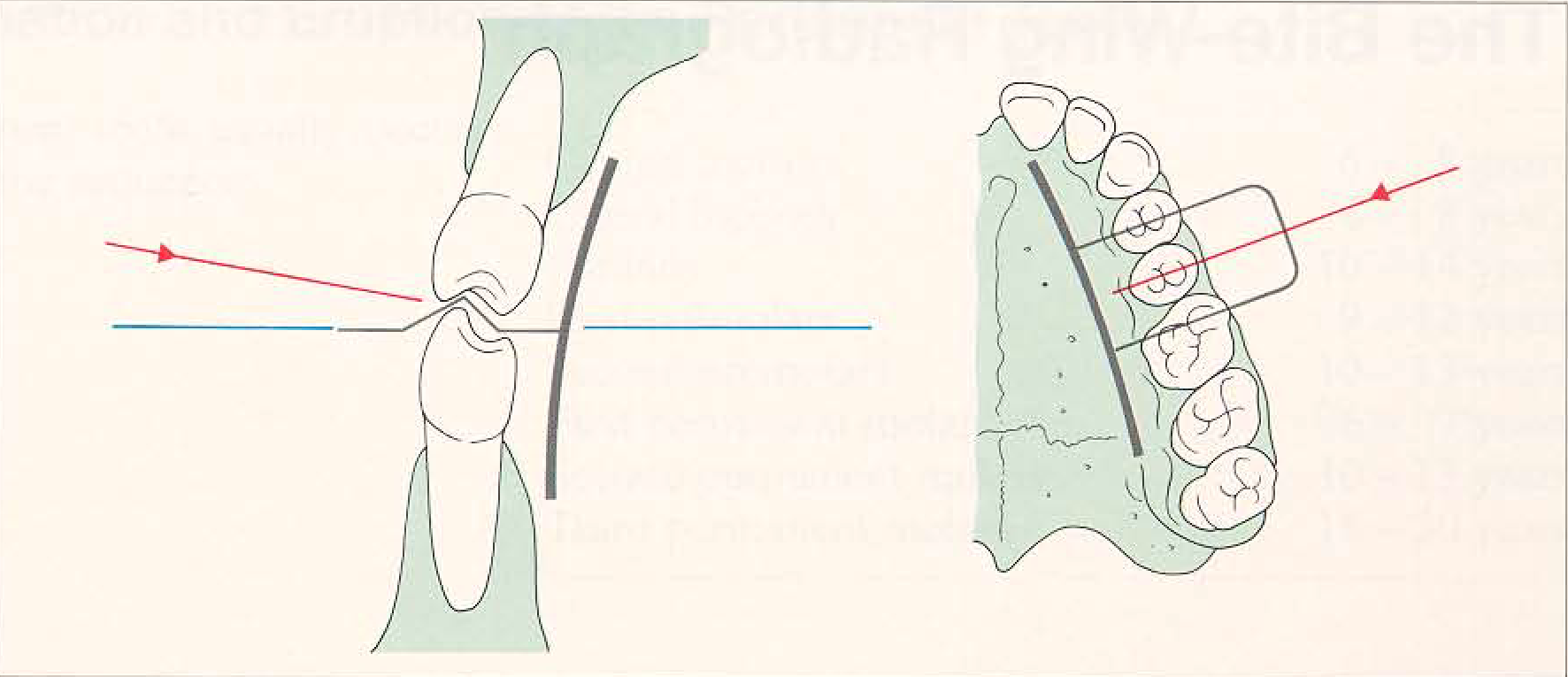
Diagram of correct film position and central ray targeting. For adolescents and adults, the long bite-wing tilm from Kodak can be used. The paper extension from the film packet must not be pulled too much. The central ray is targeted through either the maxillary second premolar or the first permanent molar.
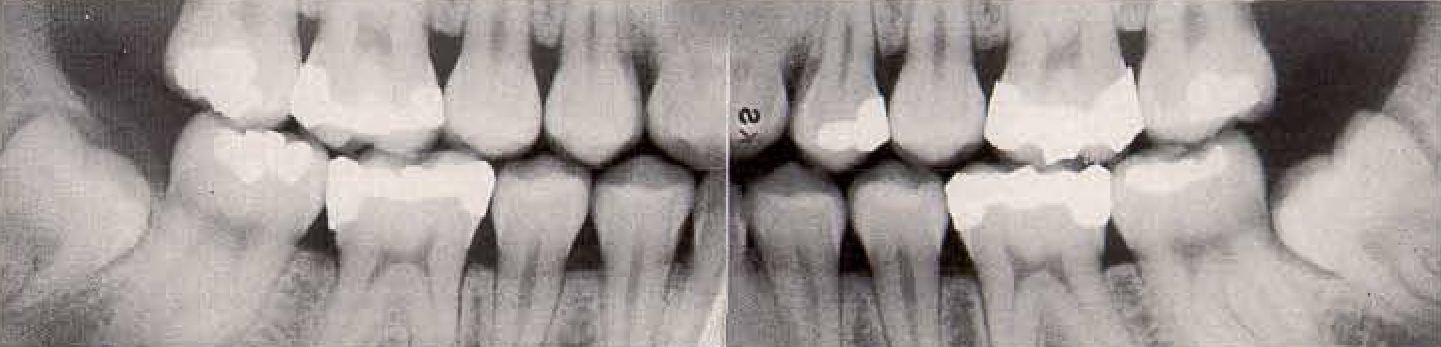
Examples. These bite-wings were taken using the long (2.5 x 5.5 cm) bite-wing film from Kodak. If the paper tab is pulled too tightly, the distal edge of the film will be pushed inferiorly when the patient bites in centric occlusion. If the film is positioned too far anteriorly, the mesial edge of the film will be pushed upward during closure. Both of these errors will result in the occlusal plane appearing oblique on the finished radiograph.
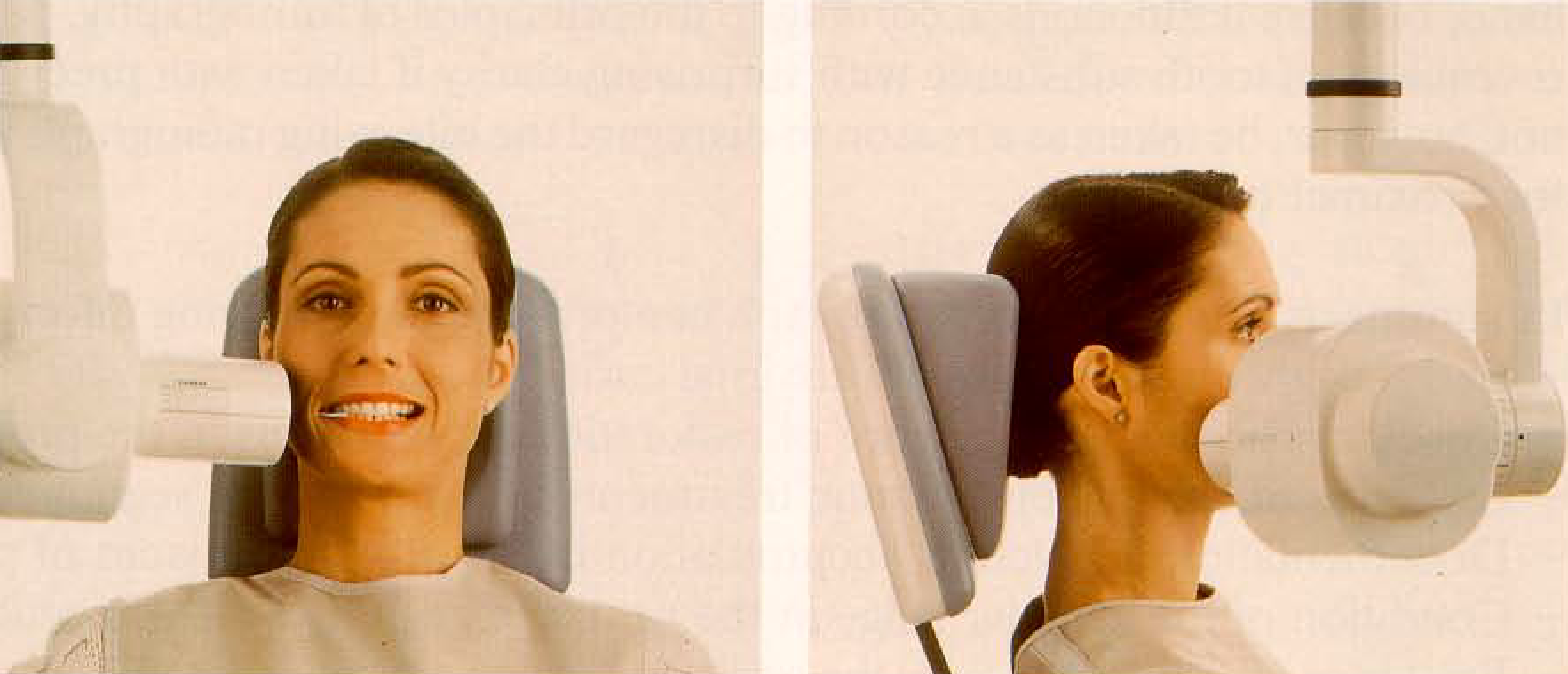
Proper central ray targeting, depicted from frontal and lateral views. Note the patient’s head position and the position of the film axis. Note also that the central ray is positioned ata5-7° angle from the horizontal plane, vertically. The horizontal targeting appears “mesial eccentric," but it is in fact perpendicular to the film surface.
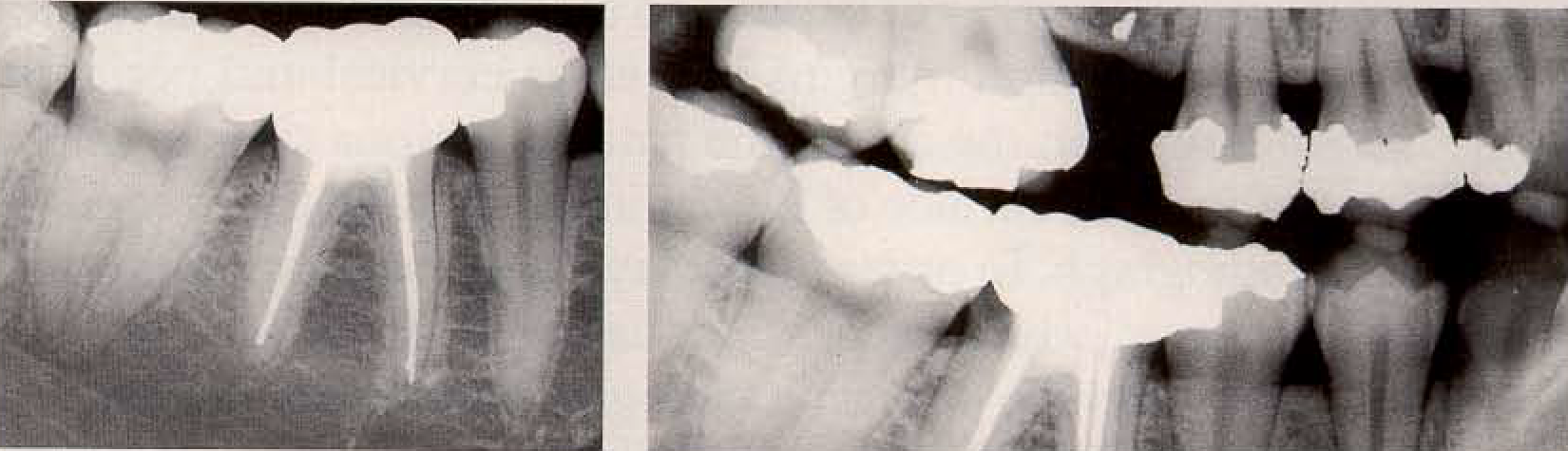
Significance of the proper targeting of the central ray for bite-wings in comparison to periapical radiographs. The bite-wing film (right) shows the superiority of the coronally targeted central ray for detection of carious lesions in the cervical area of tooth 46; compare to the periapical film (left).
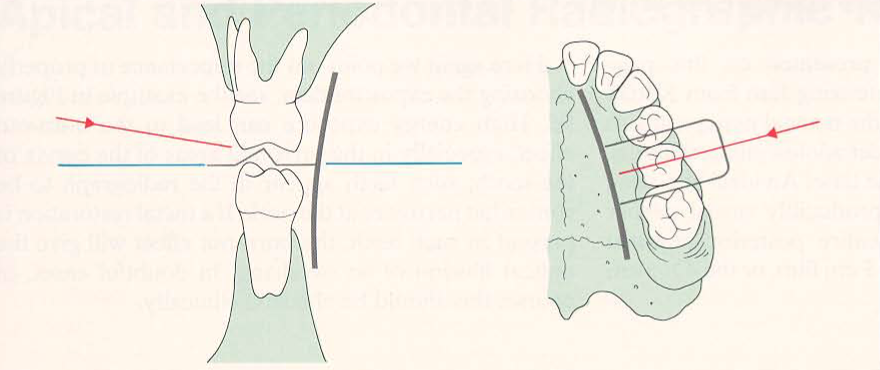
Diagram of correct film position and central ray projection. Depicted is the situation for either the child film or the normal film packet. The paper tab of the film packet must not be pulled too tightly. The central ray traverses the first or second deciduous molars.
Date added: 2022-12-17; views: 1129;